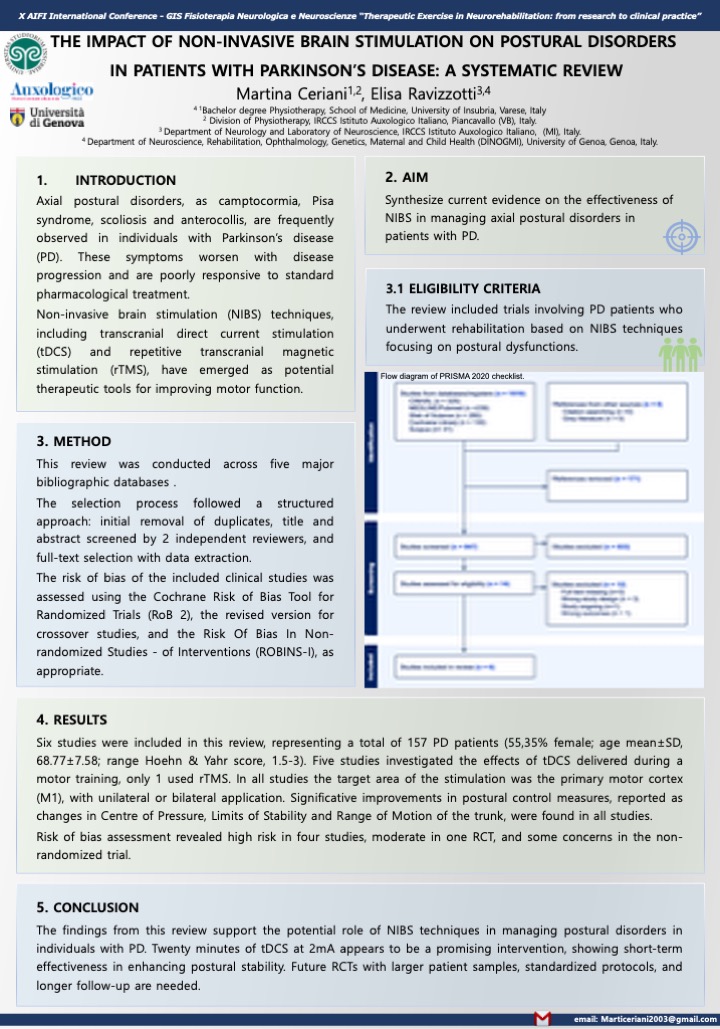
THE IMPACT OF NON-INVASIVE BRAIN STIMULATION ON POSTURAL DISORDERS IN PATIENTS WITH PARKINSON’S DISEASE: A SYSTEMATIC REVIEW
Autori
Martina Ceriani (1Bachelor degree Physiotherapy, School of Medicine, University of Insubria, Varese, Italy 2 Division of Physiotherapy, IRCCS Istituto Auxologico Italiano, Piancavallo (Verbania), Italy.)
Elisa Ravizzotti (Department of Neurology and Laboratory of Neuroscience, IRCCS Istituto Auxologico Italiano, Milan, Italy. 4 Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health (DINOGMI), University of Genoa, Genoa, Italy.)
Background and aims
Axial postural disorders, as camptocormia, Pisa syndrome, scoliosis and anterocollis, are frequently observed in individuals with Parkinson’s disease. These symptoms worsen with disease progression and are poorly responsive to standard pharmacological treatments, leading to a greater functional impairment and a significant decline in quality of life. NIBS techniques, including tDCS and rTMS, have emerged as potential therapeutic tools for improving motor function.The main purpose of this systematic review was to synthesize current evidence on the effectiveness of NIBS in managing axial postural disorders in patients with PD.
Methods
The literature search for this review was conducted across five major bibliographic databases: PubMed, the Cochrane Library, Scopus, Web of Science, and CINAHL. The search strategy, from inception to April 2024, was structured using the Problem-Intervention-Outcome. The selection process followed a structured approach: initial removal of duplicates, title and abstract screened by 2 independent reviewers, and full-text selection with data extraction. The review included trials involving adult patients with PD who underwent rehabilitation interventions based on NIBS techniques. To be eligible, studies had to assess at least one outcome related to postural alignment or postural control, in static or dynamic condition. Studies were excluded if they involved patients with a DBS implant.The risk of bias of the included clinical trial studies was assessed using the Cochrane RoB 2, the version for crossover studies, and ROBINS-I.
Results
From 1.018 records, a total of four RCTs, one cross-over study and one non-randomized clinical trial study, met the inclusion criteria, involving 157 participants with PD at a mild to moderate stage. Five studies investigated the effects of tDCS, only one utilized rTMS. In all studies the target of the intervention was M1, with unilateral or bilateral application and administration in an online setting. The control interventions showed a sham stimulation. Improvements in postural control measures reported as changes in Centre of Pressure, Limits of Stability and Range of Motion of the trunk were found in all studies. Risk of bias assessment revealed high risk in four studies, moderate in one, and some concerns in another one.
Conclusion
The findings from this review support the potential role of NIBS techniques in managing postural disorders in individuals with PD. In particular, tDCS appears to be a promising intervention, showing short-term effectiveness in enhancing postural stability. There were limitations such as small sample sizes and short follow-up periods. Future RCTs with larger patient samples, standardized protocols, and longer follow-up are needed.
REFERENCES
World Health Organization. who.int. 2023. Parkinson disease.
Tolosa E, Garrido A, Scholz SW, Poewe W. Challenges in the diagnosis of
Parkinson’s disease. Vol. 20, The Lancet Neurology. Lancet Publishing Group;
2021. pag. 385–97.
Feigin VL, Nichols E, Alam T, Bannick MS, Beghi E, Blake N, et al. Global,
regional, and national burden of neurological disorders, 1990–2016: a systematic
analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 1 maggio
2019;18(5):459–80.
Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global
burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a
systematic analysis for the Global Burden of Disease Study 2019. The Lancet
[Internet]. ottobre 2020;396(10258):1204–22. Disponibile su:
https://linkinghub.elsevier.com/retrieve/pii/S0140673620309259
Xu T, Dong W, Liu J, Yin P, Wang Z, Zhang L, et al. Disease burden of
Parkinson’s disease in China and its provinces from 1990 to 2021: findings from
the global burden of disease study 2021. Lancet Reg Health West Pac. 1 maggio
2024;46.
Ben-Shlomo Y, Darweesh S, Llibre-Guerra J, Marras C, San Luciano M, Tanner
C. The epidemiology of Parkinson’s disease. Vol. 403, The Lancet. Elsevier B.V.;
2024. pag. 283–92.
Jankovic J, Tan EK. Parkinson’s disease: Etiopathogenesis and treatment. J
Neurol Neurosurg Psychiatry. 1 agosto 2020;91(8):795–808.
Gayed I, Joseph U, Fanous M, Wan D, Schiess M, Ondo W, et al. The Impact of
DaTscan in the Diagnosis of Parkinson Disease. 2015.
Marsili L, Rizzo G, Colosimo C. Diagnostic criteria for Parkinson’s disease:
From James Parkinson to the concept of prodromal disease. Vol. 9, Frontiers in
Neurology. Frontiers Media S.A.; 2018.
Margaret M. Hoehn M and MDYM. Parkinsonism Onset, progression, and
mortality. Neurology Journals. 1998;427–42.11. 12. 13. 14. 15. 16. 17. 18. 19. 20. Movement Disorder Society Task Force report on the Hoehn and Yahr staging
scale: Status and recommendations The Movement Disorder Society Task Force
on rating scales for Parkinson’s disease | Enhanced Reader. 2004;
Goetz CG, Tilley BC, Shaftman SR, Stebbins GT, Fahn S, Martinez-Martin P, et
al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s
Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing
results. Movement Disorders. 15 novembre 2008;23(15):2129–70.
Goetz CG, Poewe W, Rascol O, Sampaio C, Stebbins GT, Counsell C, et al.
Movement Disorder Society Task Force report on the Hoehn and Yahr staging
scale: Status and recommendations. Movement Disorders. settembre
2004;19(9):1020–8.
Skorvanek M, Martinez-Martin P, Kovacs N, Rodriguez-Violante M et al.
Differences in MDS-UPDRS Scores Based on Hoehn and Yahr Stage and
Disease Duration. Mov Disord Clin Pract. 2017 Mar 11;4(4):536-544..
Chakra G. A Review of Parkinson’s Disease: Diagnosis and Treatment. Future J
Pharm Health Sci. 2023;3(4):416–25.
Leite Silva ABR, Gonçalves de Oliveira RW, Diógenes GP, de Castro Aguiar
MF, Sallem CC, Lima MPP, et al. Premotor, nonmotor and motor symptoms of
Parkinson’s Disease: A new clinical state of the art. Vol. 84, Ageing Research
Reviews. Elsevier Ireland Ltd; 2023.
Cheung TCK, Schmuckler MA. Multisensory postural control in adults:
Variation in visual, haptic, and proprioceptive inputs. Hum Mov Sci. 1 ottobre
2021;79.
Ivanenko Y, Gurfinkel VS. Human postural control. Vol. 12, Frontiers in
Neuroscience. Frontiers Media S.A.; 2018.
Carini F, Mazzola M, Fici C, Palmeri S, Messina M, Damiani P, et al. Posture and
posturology, anatomical and physiological profiles: Overview and current state
of art. Vol. 88, Acta Biomedica. Mattioli 1885 S.p.A.; 2017. pag. 11–6.
Fukunaga JY, Quitschal RM, Doná F, Ferraz HB, Ganança MM, Caovilla HH.
Postural control in Parkinson’s disease. Braz J Otorhinolaryngol.
2014;80(6):508–14.21. 22. 23. 24. 25. 26. 27. 28. 29. 30. Robinson K, Roalf DR, Cianci H, Bunting-Perry L, Dennison A, Roalf D, et al.
Falling risk factors in Parkinson’s disease. Vol. 20, NeuroRehabilitation. IOS
Press; 2005.
Allcock LM, Rowan EN, Steen IN, Wesnes K, Kenny RA, Burn DJ. Impaired
attention predicts falling in Parkinson’s disease. Parkinsonism Relat Disord.
febbraio 2009;15(2):110–5.
Sarter M, Albin RL, Kucinski A, Lustig C. Where attention falls: Increased risk
of falls from the converging impact of cortical cholinergic and midbrain
dopamine loss on striatal function. Vol. 257, Experimental Neurology. Academic
Press Inc.; 2014. pag. 120–9.
Crouse JJ, Phillips JR, Jahanshahi M, Moustafa AA. Postural instability and falls
in Parkinson’s disease. Vol. 27, Reviews in the Neurosciences. Walter de Gruyter
GmbH; 2016. pag. 549–55.
Paul SS, Sherrington C, Canning CG, Fung VSC, Close JCT, Lord SR. The
relative contribution of physical and cognitive fall risk factors in people with
Parkinson’s disease: A large prospective cohort study. Neurorehabil Neural
Repair. marzo 2014;28(3):282–90.
Borel L, Alescio-Lautier B. Posture and cognition in the elderly: Interaction and
contribution to the rehabilitation strategies. Vol. 44, Neurophysiologie Clinique.
2014. pag. 95–107.
Phenotype of postural instability:gait difficulty in Parkinson disease: relevance to
cognitive impairment and mechanism relating pathological proteins and
neurotransmitters | Enhanced Reader.
Visser M, Marinus J, Bloem BR, Kisjes H, van den Berg BM, van Hilten JJ.
Clinical tests for the evaluation of postural instability in patients with parkinson’s
disease. Arch Phys Med Rehabil. 2003 Nov;84(11):1669-74.
Jacobs J V., Horak FB, Tran VK, Nutt JG. Multiple balance tests improve the
assessment of postural stability in subjects with Parkinson’s disease. J Neurol
Neurosurg Psychiatry. 2006;77(3):322–6.
Walter Maetzler 1 JDKSJJFBRB. Quantitative wearable sensors for objective
assessment of Parkinson’s disease. Mov Disord. 12 settembre 2013;31. 32. 33. 34. 35. 36. 37. 38. 39. 40. Ferreira-Peruzzo Silvia AparecidaORCID Icon CCHFIZMBIRPRMRPI&
THAGI. Static posturography analysis for postural instability in patients with
Parkinson’s disease. Int J Neurosci. 2023;
Ferraris C, Votta V, Nerino R, Chimienti A, Priano L, Mauro A. At-home
assessment of postural stability in parkinson’s disease: a vision-based approach. J
Ambient Intell Humaniz Comput. 1 maggio 2024;15(5):2765–78.
Shirahige L, Leimig B, Baltar A, Bezerra A, de Brito CVF, do Nascimento YSO,
et al. Classification of Parkinson’s disease motor phenotype: a machine learning
approach. J Neural Transm. 1 dicembre 2022;129(12):1447–61.
Abe K, Uchida Y, Notani M. Camptocormia in Parkinson’s disease. Parkinsons
Dis. 2010 Jun 30;2010:267640.
Margraf NG, Granert O, Hampel J, Wrede A, Schulz-Schaeffer WJ, Deuschl G.
Clinical Definition of Camptocormia in Parkinson’s Disease. Mov Disord Clin
Pract. 2016 Oct 11;4(3):349-357.
Tinazzi M, Geroin C, Bhidayasiri R, Bloem BR, Capato T, Djaldetti R et al.
International Parkinson and Movement Disorders Society Task Force on
Postural Abnormalities. Task Force Consensus on Nosology and Cut-Off Values
for Axial Postural Abnormalities in Parkinsonism. Mov Disord Clin Pract. 2022
May 9;9(5):594-603. .
Furusawa Y, Mukai Y, Kobayashi Y, Sakamoto T, Murata M. Role of the
external oblique muscle in upper camptocormia for patients with Parkinson’s
disease. Vol. 27, Movement Disorders. 2012. pag. 802–3.
Fasano A, Geroin C, Berardelli A, Bloem BR, Espay AJ, Hallett M, Lang AE,
Tinazzi M. Diagnostic criteria for camptocormia in Parkinson’s disease: A
consensus-based proposal. Parkinsonism Relat Disord. 2018 Aug;53:53-57.
Srivanitchapoom P, Hallett M. Camptocormia in Parkinson’s disease: definition,
epidemiology, pathogenesis and treatment modalities. J Neurol Neurosurg
Psychiatry. 2016 Jan;87(1):75-85. doi: 10.1136/jnnp-2014-310049. Epub 2015
Apr 20.
Tinazzi M, Geroin C, Gandolfi M, Smania N, Tamburin S, Morgante F, Fasano
A. Pisa syndrome in Parkinson’s disease: An integrated approach from
pathophysiology to management. Mov Disord. 2016 Dec;31(12).41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. Miletic V. Pisa syndrome in Parkinson’s disease: diagnostic and management
challenges. Research and Reviews in Parkinsonism. 2016;6:29-35.
Geroin C, Artusi CA, Gandolfi M, Zanolin E, Ceravolo R, Capecci M, et al.
Does the Degree of Trunk Bending Predict Patient Disability, Motor
Impairment, Falls, and Back Pain in Parkinson’s Disease? Front Neurol. 31
marzo 2020;11.
Tinazzi M, Fasano A, Geroin C, Morgante F, Ceravolo R, Rossi S et al. Italian
Pisa Syndrome Study Group. Pisa syndrome in Parkinson disease: An
observational multicenter Italian study. Neurology. 2015 Nov 17;85(20):1769-
79..
Vitale C, Falco F, Trojano L, Erro R, Moccia M, Allocca R, et al.
Neuropsychological correlates of Pisa syndrome in patients with Parkinson’s
disease. Acta Neurol Scand. 1 agosto 2016;134(2):101–7.
Cannas A, Solla P, Floris G, Tacconi P, Serra A, Piga M, Marrosu F, Marrosu
MG. Reversible Pisa syndrome in patients with Parkinson’s disease on
dopaminergic therapy. J Neurol. 2009 Mar;256(3):390-5.
Artusi CA, Montanaro E, Tuttobene S, Romagnolo A, Zibetti M, Lopiano L.
Pisa Syndrome in Parkinson’s Disease Is Associated With Specific Cognitive
Alterations. Front Neurol. 2019 May 31;10:577.
Lai Y, Song Y, Su D, Wang L, Zhang C, Sun B, et al. Pallidal stimulation as
treatment for camptocormia in Parkinson’s disease. NPJ Parkinsons Dis. 1
dicembre 2021;7(1).
Chieng LO, Madhavan K, Wang MY. Deep brain stimulation as a treatment for
Parkinson’s disease related camptocormia. Vol. 22, Journal of Clinical
Neuroscience. Churchill Livingstone; 2015. pag. 1555–61.
Ando Y, Fujimoto K ichi, Ikeda K, Utsumi H, Okuma Y, Oka H, et al. Postural
Abnormality in Parkinson’s Disease: A Large Comparative Study With General
Population. Mov Disord Clin Pract. 1 marzo 2019;6(3):213–21.
Balestrino R, Schapira AHV. Parkinson disease. Vol. 27, European Journal of
Neurology. Blackwell Publishing Ltd; 2020. pag. 27–42.
Sprenger F, Poewe W. Management of motor and non-motor symptoms in
parkinson’s disease. Vol. 27, CNS Drugs. 2013. pag. 259–72.52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. Hariz M, Blomstedt P. Deep brain stimulation for Parkinson’s disease. Vol. 292,
Journal of Internal Medicine. John Wiley and Sons Inc; 2022. pag. 764–78.
N. Bolognini GV. Stimolare il cervello – manuale di stimolazione cerebrale non
invasiva . Il Mulino, curatore. 2015.
Kesikburun S. Non-invasive brain stimulation in rehabilitation. Turk J Phys Med
Rehabil. 2022 Mar 1;68(1):1-8.
Lefaucheur JP, André-Obadia N, Antal A, Ayache SS, Baeken C, Benninger DH,
et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial
magnetic stimulation (rTMS). Vol. 125, Clinical Neurophysiology. Elsevier
Ireland Ltd; 2014. pag. 2150–206.
Lefaucheur JP, Aleman A, Baeken C, Benninger DH, Brunelin J, Di Lazzaro V,
et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial
magnetic stimulation (rTMS): An update (2014–2018). Vol. 131, Clinical
Neurophysiology. Elsevier Ireland Ltd; 2020. pag. 474–528.
Schulz R, Gerloff C, Hummel FC. Non-invasive brain stimulation in
neurological diseases. Vol. 64, Neuropharmacology. 2013. pag. 579–87.
Aderinto N, Olatunji G, Muili A, Kokori E, Edun M, Akinmoju O, et al. A
narrative review of non-invasive brain stimulation techniques in neuropsychiatric
disorders: current applications and future directions. Vol. 60, Egyptian Journal of
Neurology, Psychiatry and Neurosurgery. Springer Science and Business Media
Deutschland GmbH; 2024.
He W, Fong PY, Leung TWH, Huang YZ. Protocols of non-invasive brain
stimulation for neuroplasticity induction. Vol. 719, Neuroscience Letters.
Elsevier Ireland Ltd; 2020.
Von Bernhardi R, Eugenín-Von Bernhardi L, Eugenín J. What is neural
plasticity? In: Advances in Experimental Medicine and Biology. Springer New
York LLC; 2017. pag. 1–15.
Kania BF, Wrońska D, Zięba D. Introduction to Neural Plasticity Mechanism. J
Behav Brain Sci. 2017;07(02):41–9.
Zewdie E, Ciechanski P, Kuo HC, Giuffre A, Kahl C et al. Safety and tolerability
of transcranial magnetic and direct current stimulation in children: Prospective63. 64. 65. 66. 67. 68. 69. 70. 71. single center evidence from 3.5 million stimulations. Brain Stimul. 2020 May-
Jun;13(3):565-575..
Matsumoto H, Ugawa Y. Adverse events of tDCS and tACS: A review. Vol. 2,
Clinical Neurophysiology Practice. Elsevier B.V.; 2017. pag. 19–25.
McClintock SM, Reti IM, Carpenter LL, McDonald WM, Dubin M, Taylor SF et
al. National Network of Depression Centers rTMS Task Group; American
Psychiatric Association Council on Research Task Force on Novel Biomarkers
and Treatments. Consensus Recommendations for the Clinical Application of
Repetitive Transcranial Magnetic Stimulation (rTMS) in the Treatment of
Depression. J Clin Psychiatry. 2018 Jan/Feb;79(1).
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et
al. The PRISMA 2020 statement: An updated guideline for reporting systematic
reviews. Vol. 372, The BMJ. BMJ Publishing Group; 2021.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I et al. RoB
2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019 Aug
28;
Revised Cochrane risk-of-bias tool for randomized crossover trials SHORT
VERSION (CRIBSHEET).
The Risk Of Bias In Non-randomized Studies-of Interventions (ROBINS-I)
assessment tool (version for cohort-type studies) ROBINS-I tool (Stage I): At
protocol stage Specify the review question.
Yang C, Xu Y, Feng X, Wang B, Du Y, Wang K, Lü J, Huang L, Qian Z, Wang
Z, Chen N, Zhou J, Zhang C, Liu Y. Transcranial Temporal Interference
Stimulation of the Right Globus Pallidus in Parkinson’s Disease. Mov Disord.
2024 Aug 12. .
Romero JP, Moreno-Verdú M, Arroyo-Ferrer A, Serrano JI, Herreros-Rodríguez
J, García-Caldentey J, et al. Clinical and neurophysiological effects of bilateral
repetitive transcranial magnetic stimulation and EEG-guided neurofeedback in
Parkinson’s disease: a randomized, four-arm controlled trial. J Neuroeng
Rehabil. 1 dicembre 2024;21(1).
Beretta VS, Orcioli-Silva D, Zampier VC, Moraca GAG, Pereira MP, Gobbi
LTB, et al. Eight sessions of transcranial electrical stimulation for postural72. 73. 74. 75. 76. 77. 78. 79. response in people with Parkinson’s disease: A randomized trial. Gait Posture. 1
ottobre 2024;114:1–7.
Marcus Grobe-Einsler ALJWOK. RTMS of the Cerebellum Using an
Accelerated Stimulation Protocol Improved Gait in Parkinson’s Disease.
Neurorehabil Neural Repair. luglio 2024;539–50.
TRANSCRANIAL DIRECT CURRENT STIMULATION (t-DCS) AS ADD-
ON TO NEUROREHABILITATION OF PISA SYNDROME IN
PARKINSON DISEASE. Clinicaltrials.gov. 1 gennaio 2020;0(0).
Qi J, KG, SK, SS, MM. The effects of non-invasive transcranial brain current
stimulation (tDCS) on posture over stable and unstable surfaces in people with
Parkinson’s: a randomised doubleblind sham-controlled crossover study. J
Parkinsons Dis. 1 gennaio 2019;9(1):190.
Kaut O, GEM. Noninvasive brain stimulation improves motor function in
Parkinson’s disease. Neurologie und rehabilitation. 1 gennaio 2023;23(0).
Rashid-Lopez R, CGAJ, MGP, SF ez, FL, LSE, SF, CCF, REG, ERR, GRJJ.
Marked improvement of postural and gait disturbances in Parkinson’s disease
with bilateral primary motor area intermittent theta-burst stimulation may be
linked to increased putamen-cortico-cerebellar functional connectivity: a case
report. Brain stimulation2. 1 gennaio 2023;16(1):271–2.
Rashid-López R, MGP, CGÁJ, SFFL, CCF, SF et al. Bilateral primary motor
area intermittent theta-burst stimulation may alleviate gait and postural
disturbances in Parkinson’s disease patients by astrocytic modulation, caudate
volume changes, and increased functional neuroplasticity. Parkinsonism Relat
Disord. 1 gennaio 2024;123(0).
Radder DLM, Lígia Silva de Lima A, Domingos J, Keus SHJ, van Nimwegen M,
Bloem BR, de Vries NM. Physiotherapy in Parkinson’s Disease: A Meta-Analysis
of Present Treatment Modalities. Neurorehabil Neural Repair. 2020
Oct;34(10):871-880.).
Legutke BR, Gobbi LTB, Orcioli-Silva D, Santos PCR dos, Moraca GAG,
Vitório R, et al. Transcranial direct current stimulation suggests not improving
postural control during adapted tandem position in people with Parkinson’s
disease: A pilot study. Behavioural Brain Research. 24 agosto 2023;452.80. 81. 82. 83. 84. 85. 86. 87. Beretta VS, Vitório R, Nóbrega-Sousa P, Conceição NR, Orcioli-Silva D, Pereira
MP, et al. Effect of Different Intensities of Transcranial Direct Current
Stimulation on Postural Response to External Perturbation in Patients With
Parkinson’s Disease. Neurorehabil Neural Repair. 1 novembre
2020;34(11):1009–19.
Beretta VS, Orcioli-Silva D, Conceição NR, Nóbrega-Sousa P, Pereira MP,
Gobbi LTB, et al. tDCS application for postural control in Parkinson’s disease:
Effects are associated with baseline characteristics. Parkinsonism Relat Disord. 1
dicembre 2021;93:62–5.
De Icco R, Putortì A, Allena M, Avenali M, Dagna C, Martinelli D, et al. Non-
Invasive Neuromodulation in the Rehabilitation of Pisa Syndrome in Parkinson’s
Disease: A Randomized Controlled Trial. Front Neurol. 14 aprile 2022;13.
Yitayeh A, Teshome A. The effectiveness of physiotherapy treatment on balance
dysfunction and postural instability in persons with Parkinson’s disease: A
systematic review and meta-analysis. BMC Sports Sci Med Rehabil. 11 febbraio
2016;8(1).
Palheta De Lima K, Nascimento Da Silva C, Ferreira De Seixas N, De M,
Maneschy S, Lima N, et al. Effect of resistance training on balance and postural
control in people with Parkinson’s: A systematic review. Vol. 56, Rev Cient Soc
Esp Enferm Neurol. 2022.
Coelho DB, de Oliveira CEN, Guimarães MVC, Ribeiro de Souza C, dos Santos
ML, de Lima-Pardini AC. A systematic review on the effectiveness of
perturbation-based balance training in postural control and gait in Parkinson’s
disease. Vol. 116, Physiotherapy (United Kingdom). Elsevier Ltd; 2022. pag. 58–
71.
Bath JE, Wang DD. Unraveling the threads of stability: A review of the
neurophysiology of postural control in Parkinson’s disease. Vol. 21,
Neurotherapeutics. Elsevier B.V.; 2024.
Fatemeh Ehsani ASMZRHSJ. The effects of cerebellar transcranial direct current
stimulation on static and dynamic postural stability in older individuals: a
randomized double-blind sham-controlled study. European Journal of
Neuroscience. ottobre 2017;