Red flags per lo screening di neoplasie in pazienti con cervicalgia: una scoping review
Autori
Occhetto Beatrice, PT [Department of General Practice, Erasmus MC, University Medical Centre, Rotterdam, The Netherlands]
Ballesio Martina, PT [Department of General Practice, Erasmus MC, University Medical Centre, Rotterdam, The Netherlands]
Mourad Firas,PT, MSc, PhD [Department of Health, LUNEX University of applied sciences, 50, Avenue du Parc des Sports, 4671 Differdange, Luxembourg. Luxembourg Health and Sport Sciences Research Institute A.s.b.l., 50, Avenue du Parc des Sports, 4671 Differdange, Luxembourg]
Trucco Marco, PT, MSc [School of Physiotherapy, University of Turin School of Medicine, Turin, Italy. Presidio Sanitario San Camillo di Torino, Turin, Italy]
Maselli Filippo,PT, MSc, PhD [Department of Human Neurosciences, Sapienza University of Rome, Rome, Italy. Sovrintendenza Sanitaria Regionale Puglia, INAIL, Bari, Italy]
Chiarotto Alessandro, PT, MSc, PhD [Department of General Practice, Erasmus MC, University Medical Centre, Rotterdam, The Netherlands]
Feller Daniel [Department of General Practice, Erasmus MC, University Medical Centre, Rotterdam, The Netherlands]
Background and aims
Neck pain is a highly prevalent condition that leads to considerable pain, disability, and economic costs at a societal level (1,2). It represents a major burden for the affected people’s quality of life, their caregivers, and healthcare systems. (2) A systematic analysis of the Global Burden of Disease Study 2021 reported that, in 2020, neck pain affected approximately 203 million people worldwide, making it the third most burdensome condition amongst musculoskeletal disorders (3). Although rare, neoplastic causes of neck pain must be promptly identified to ensure timely referral and management (4–6). Red flags are clinical indicators intended to support clinicians in detecting such serious conditions in early stages (7–9). This scoping review systematically maps and summarizes the literature on red flags for tumours in patients presenting with neck pain in primary care, highlighting evidence gaps and priorities for future research.
Methods
A comprehensive search across four databases up to May 2024 targeted studies on patients of any age or gender presenting with neck pain as the primary complaint and a final diagnosis of a tumour. Only studies conducted in primary care were included, with no time or geographical restrictions. Data were synthesized quantitatively and thematically.
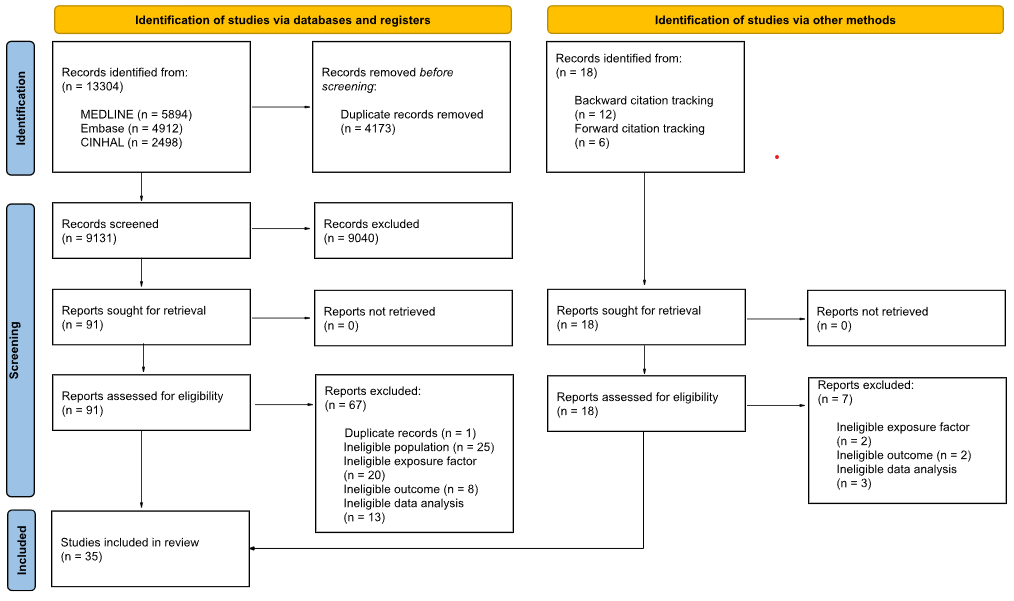
Results
From 9 054 initial records, 24 studies met the inclusion criteria, all being case reports. The most frequently reported red flags were severe neck pain, which may become progressive and constant, neurological signs and symptoms, and nocturnal neck pain. However, inconsistencies in reporting were observed: many commonly discussed red flags were absent from case reports, while some red flags highlighted in case reports are not extensively covered in the literature.
Conclusion
Evidence on red flags for tumours in patients with neck pain in primary care remains fragmented. While certain red flags were frequently reported, their clinical utility is limited by inconsistent reporting and a lack of robust evidence. Further research is needed to standardize red flags and assess their diagnostic accuracy to improve early tumour detection in patients with neck pain.
REFERENCES
- Mourad F, Giovannico G, Maselli F, Bonetti F, Fernández de las Peñas C, Dunning J. Basilar impression presenting as intermittent mechanical neck pain: a rare case report. BMC Musculoskelet Disord. 11 gennaio 2016; 17:7.
- Safiri S, Kolahi AA, Hoy D, Buchbinder R, Mansournia MA, Bettampadi D, et al. Global, regional, and national burden of neck pain in the general population, 1990-2017: systematic analysis of the Global Burden of Disease Study 2017. BMJ. 26 marzo 2020;368:m791.
- Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet. 17 ottobre 2020;396(10258):1204–22.
- GBD 2021 Neck Pain Collaborators. Global, regional, and national burden of neck pain, 1990-2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. marzo 2024;6(3):e142–55.
- Masters S. Acute cervical spine pain in primary care. Aust J Gen Pract. 1 novembre 2023;52(11):745–50.
- Mourad F, Cataldi F, Patuzzo A, Tunnera S, Dunning J, Fernández-de-las-Peñas C, et al. Craniopharyngioma in a young woman with symptoms presenting as mechanical neck pain associated with cervicogenic headache: a case report. Physiother Theory Pract. 2021;37(4):549–58.
- Finucane LM, Downie A, Mercer C, Greenhalgh SM, Boissonnault WG, Pool-Goudzwaard AL, et al. International Framework for Red Flags for Potential Serious Spinal Pathologies. J Orthop Sports Phys Ther. luglio 2020;50(7):350–72.
- Feller D, Chiarotto A, Koes B, Maselli F, Mourad F. Red flags for potential serious pathologies in people with neck pain: a systematic review of clinical practice guidelines. Arch Physiother. 2024;14:105–15.
- Maselli F, Palladino M, Barbari V, Storari L, Rossettini G, Testa M. The diagnostic value of Red Flags in thoracolumbar pain: a systematic review. Disabil Rehabil. aprile 2022;44(8):1190–206.