Red flags per patologie gravi del rachide cervicale: una revisione sistematica di linee guida
Red flags for potential serious pathologies in people with neck pain: a systematic review of clinical practice guidelines
Autori
Feller Daniel (Department of General Practice, Erasmus MC, University Medical Centre, Rotterdam, The Netherlands)
Chiarotto Alessandro (Department of General Practice, Erasmus MC, University Medical Centre, Rotterdam, The Netherlands)
Koes Bart (Department of General Practice, Erasmus MC, University Medical Centre, Rotterdam, The Netherlands)
Maselli Filippo (Department of Human Neurosciences, Sapienza University of Rome, Rome, Italy)
Mourad Firas (Department of Health, LUNEX 50, Avenue du Parc des Sports, 4671 Differdange, Luxembourg)
Introduction
Although benign in most patients, it is estimated that 1% of neck pain can be the early manifestation of severe pathologies, such as malignancy and cervical arterial pathology. As standard practice, red flags (i.e., items from a patient’s medical history and clinical examination potentially associated with a higher risk of serious conditions) have been used to guide clinicians in identifying serious cervical pathology. 1,2 To the best of the authors’ knowledge, no systematic review has been published investigating the recommended red flags for neck pain in clinical practice guidelines. Furthermore, knowledge of which study design the red flags recommendations were based on may help clinicians to value the recommendations’ strength. Therefore, we aimed to: 1) identify red flags to triage serious pathologies recommended in international clinical practice guidelines for neck pain, 2) evaluate the consistency in red flags recommendations across guidelines, and 3) investigate the strength of evidence, including on which study design the recommendations are based on.
Methods
The study protocol was registered a priori on MedRxiv. 3 Without time and languegae restriction, we searched for guidelines focusing on specific and non-specific neck pain in MEDLINE (via PubMed), EMBASE, and PEDro electronic databases on 09/06/2023. Guidelines were also searched through forward and backward citation tracking strategies (Web of Science on 12/07/2023), by consulting experts in the field (top 10 experts on neck pain according to ExpertScape.com on 15/07/2023), and by checking guideline organization databases (e.g., the “Canadian Medical Association Infobase of clinical practice guidelines” and the “Istituto Superiore Sanità – Sistema Nazionale Linee Guida”). Two reviewers performed independently the study selection and data extraction phases. We calculated Fleiss’ kappa to evaluate the consistency among guidelines recommendations. 4 Additionally, to summarize the recommendations to triage serious pathologies and the study designs to support recommendations, we computed descriptive statistics (absolute and relative frequencies) and reported the results narratively.
Results
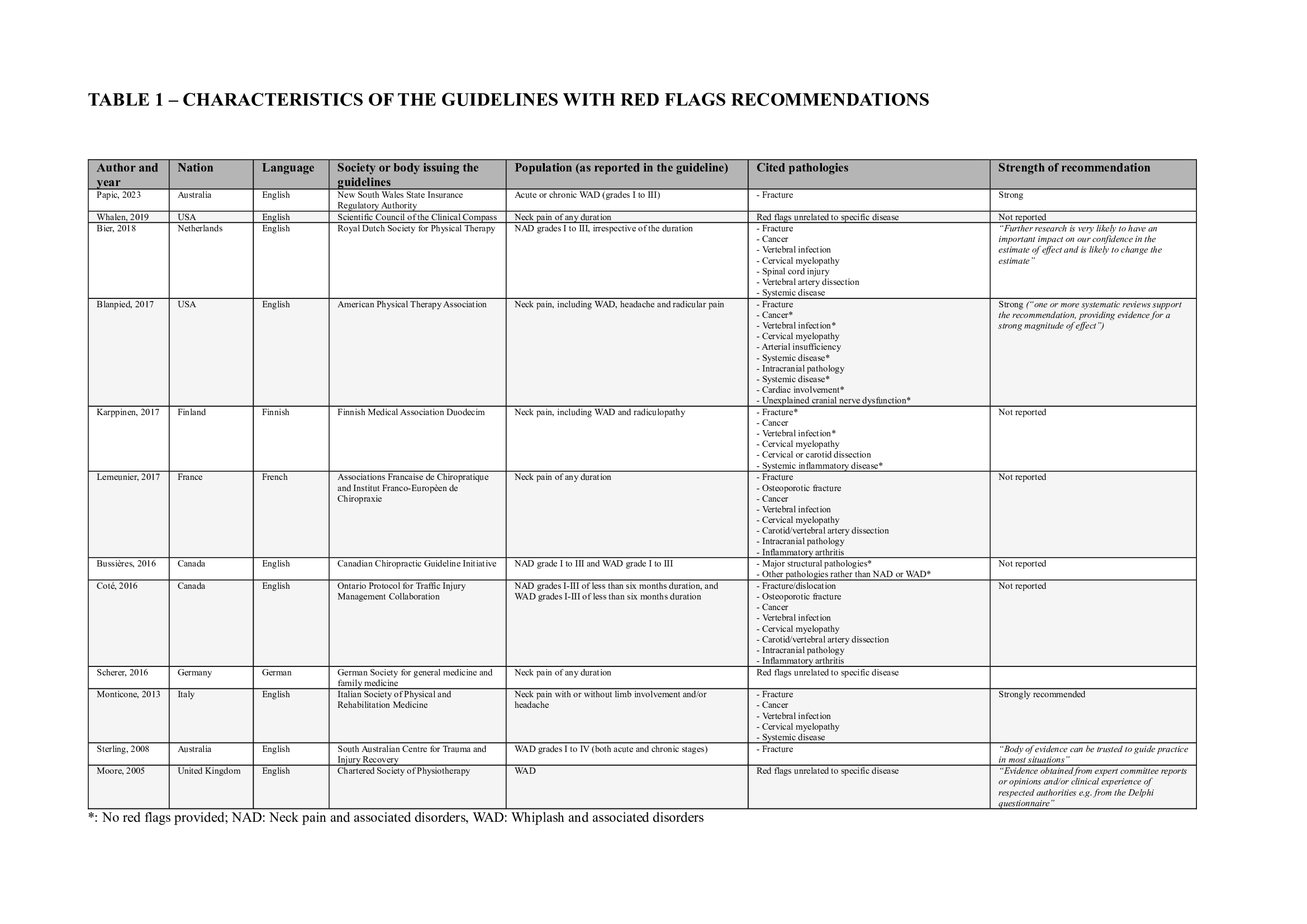
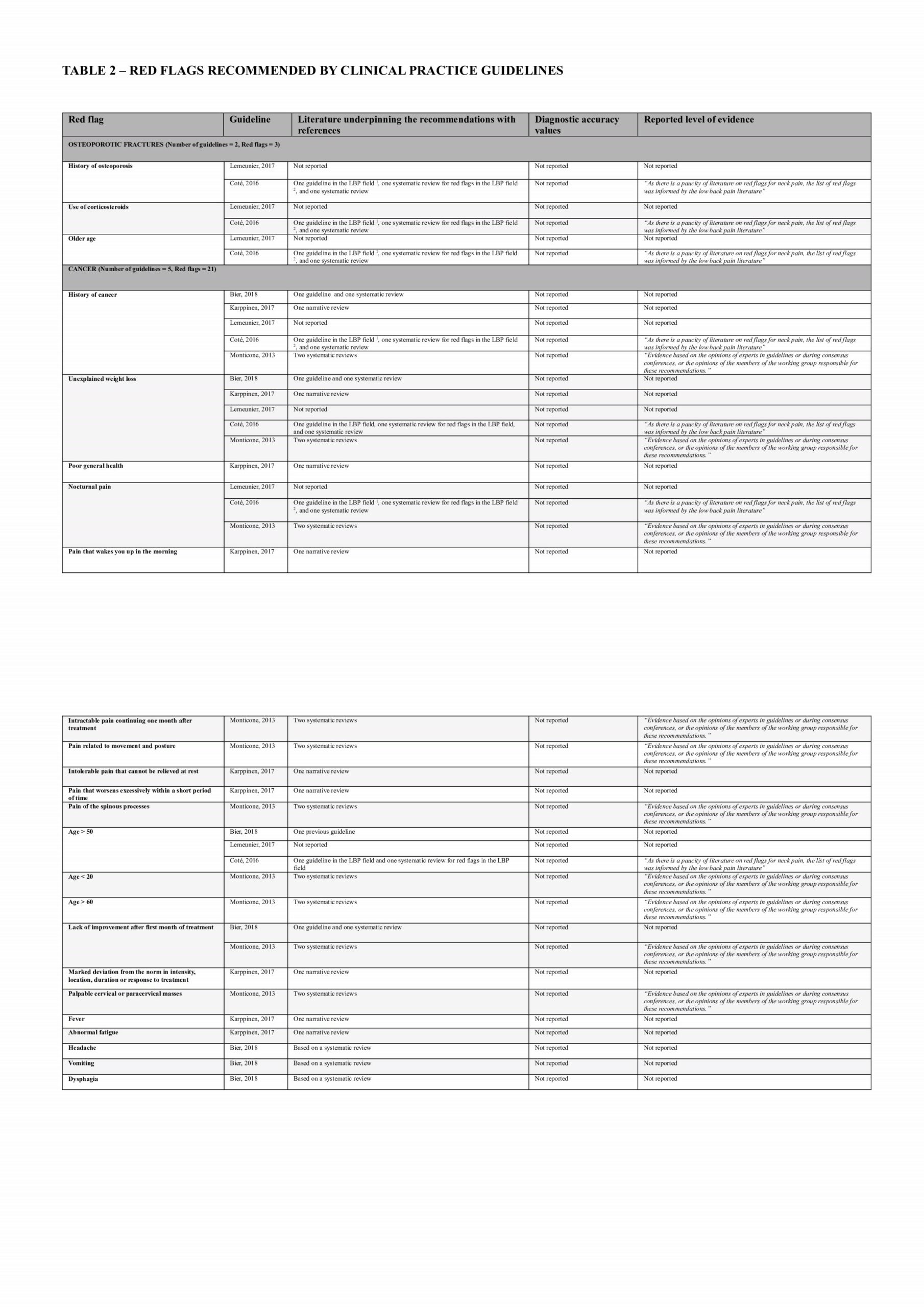
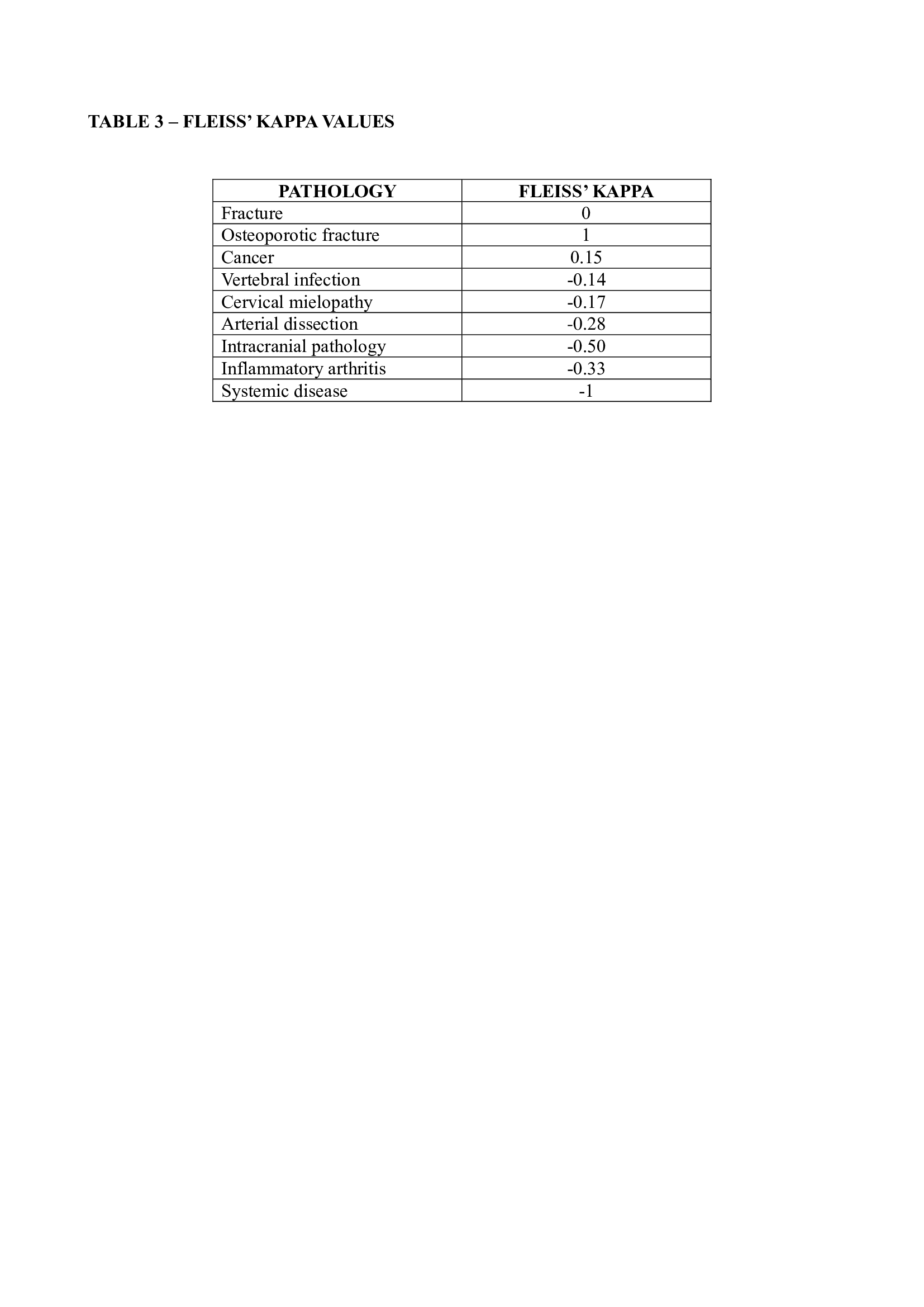
We included 29 guidelines, 12 of which provided information on red flags to screen for serious pathologies (3 for whiplash-associated disorders, 5 for neck pain and associated disorders grade I to III, and 4 for mixed populations) (Table 1). We identified a total of 114 red flags in the guidelines related to fracture, cancer, vertebral infection, myelopathy, spinal cord injury, artery dissection, intracranial pathology, inflammatory arthritis, other systemic diseases, and conditions not related to a specific condition. Overall, there is limited consensus among guidelines regarding red flags for serious pathologies, except for cancer (slight agreement with a Fleiss Kappa of 0.15) and osteoporotic fractures (perfect agreement with a Fleiss’ Kappa of 1) (Table 2 and Table 3). Among all the red flags, only the Canadian C-spine rules for fractures were based on systematic reviews and supported by diagnostic test accuracy values (sensitivity ranging from 90% to 100%; specificity ranging from 42.5% to 45.1%). 10 The remaining red flags were mainly supported by case reports and case series that did not provide direct information on their diagnostic accuracy.
Discussion and Conclusion
We found that only a few red flags were consistently reported by all the included guidelines (Table 3). Among all the red flags, only the Canadian C-spine rule could be reliably used in clinical practice. All the other red flags have limitations in terms of applicability and diagnostic predictivity, indicating a gap in the literature that should be addressed in future research. This includes conducting secondary studies to systematically summarize the available red flags and primary studies to determine the diagnostic accuracy of signs and symptoms that may suggest a serious medical condition. According to the current limitations of the evidence, clinicians should use the red flags mentioned in the guidelines cautiously and integrate them into a sound clinical reasoning process. Accordingly, when combined within a broad clinical-reasoning framework to determine the level of suspicion about serious pathology, red flags may help clinicians make the best judgment on the appropriate clinical action in a continuous monitoring process. 2
REFERENCES
- Rushton A, Carlesso LC, Flynn T, et al. International Framework for Examination of the Cervical Region for Potential of Vascular Pathologies of the Neck Prior to Musculoskeletal Intervention: International IFOMPT Cervical Framework. J Orthop Sports Phys Ther. 2023;53(1):7-22. doi:10.2519/jospt.2022.11147
- Heick J, Lazaro RT, eds. Goodman and Snyder’s Differential Diagnosis for Physical Therapists: Screening for Referral. 7th edition. Elsevier; 2022.
- Feller D, Chiarotto A, Koes B, Maselli F, Mourad F. Red flags for potential serious pathologies masquerading as musculoskeletal neck pain: a protocol for a systematic review of clinical practice guidelines. Published online June 22, 2023:2023.06.20.23291691. doi:10.1101/2023.06.20.23291691
- Fleiss JL. Measuring nominal scale agreement among many raters. Psychological Bulletin. 1971;76:378-382. doi:10.1037/h0031619
- Bier JD, Scholten-Peeters WGM, Staal JB, et al. Clinical Practice Guideline for Physical Therapy Assessment and Treatment in Patients With Nonspecific Neck Pain. Phys Ther. 2018;98(3):162-171. doi:10.1093/ptj/pzx118
- Whalen W, Farabaugh RJ, Hawk C, et al. Best-Practice Recommendations for Chiropractic Management of Patients With Neck Pain. J Manipulative Physiol Ther. 2019;42(9):635-650. doi:10.1016/j.jmpt.2019.08.001
- Label de la HAS – Évaluation du patient atteint de cervicalgie et prise de décision thérapeutique en chiropraxie. Haute Autorité de Santé. https://www.has-sante.fr/jcms/c_2803360/fr/label-de-la-has-evaluation-du-patient-atteint-de-cervicalgie-et-prise-de-decision-therapeutique-en-chiropraxie
- Scherer M, Chenot JF. Deutsche Gesellschaft für Allgemeinmedizin und Familienmedizin. Published online 2016.
- Monticone M, Iovine R, de Sena G, et al. The Italian Society of Physical and Rehabilitation Medicine (SIMFER) recommendations for neck pain. G Ital Med Lav Ergon. 2013;35(1):36-50.
- Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Worthington JR. A study to develop clinical decision rules for the use of radiography in acute ankle injuries. Annals of Emergency Medicine. 1992;21(4):384-390. doi:10.1016/S0196-0644(05)82656-3
- Saragiotto BT, Maher CG, Lin CC, Verhagen AP, Goergen S, Michaleff ZA. Canadian C‐spine rule and the National Emergency X‐Radiography Utilization Study (NEXUS) for detecting clinically important cervical spine injury following blunt trauma. Cochrane Database Syst Rev. 2018;2018(4):CD012989. doi:10.1002/14651858.CD012989