Passato, presente e futuro della teleriabilitazione in ambito cardiologico: revisione sistematica della letteratura
Past, present and future of Cardiac Telerehabilitation: a sistematic review
Autori
Garofano Marina [University of Cagliari and Department of Medicine, Surgery and Dentistry, University of Salerno, Italy]
Vecchione Carmine [Department of Medicine, Surgery and Dentistry, University of Salerno, Italy]
Calabrese Mariaconsiglia [Department of Medicine, Surgery and Dentistry, University of Salerno, Italy]
Rusciano Maria Rosaria [Department of Medicine, Surgery and Dentistry, University of Salerno, Italy]
Carrizzo Albino [Department of Medicine, Surgery and Dentistry, University of Salerno, Italy]
Galasso Gennaro [Department of Medicine, Surgery and Dentistry, University of Salerno, Italy]
Bramanti Placido [University eCampus, Novedrate, Italy]
Corallo Francesco [Centro Neurolesi Bonino Pulejo, Messina, Italy,]
Ciccarelli Michele [Department of Medicine, Surgery and Dentistry, University of Salerno, Italy]
Bramanti Alessia [Department of Medicine, Surgery and Dentistry, University of Salerno, Italy]
Introduction
Among chronic diseases, Cardiovascular Diseases (CVD) are associated with very high rates of re-hospitalization and mortality worldwide. The complexity of these pathologies requires frequent access at hospital facilities in order to allow multidisciplinary assessments and for the execution of diagnostic tests. The guidelines, also, emphasize the importance of Cardiac Rehabilitation (CR) programs, which have demonstrated a favourable effect on outcomes, so Cardiac Telerehabilitation (CTR) could represent an innovative health care delivery model that support more patient-centered care in order to meet health needs more effectively. The aim of our review is studying how technologies used in rehabilitation have changed over time and also understanding what type of rehabilitation program have been used in telerehabilitation to answer the complex health needs of people with cardiovascular disease.
Methods
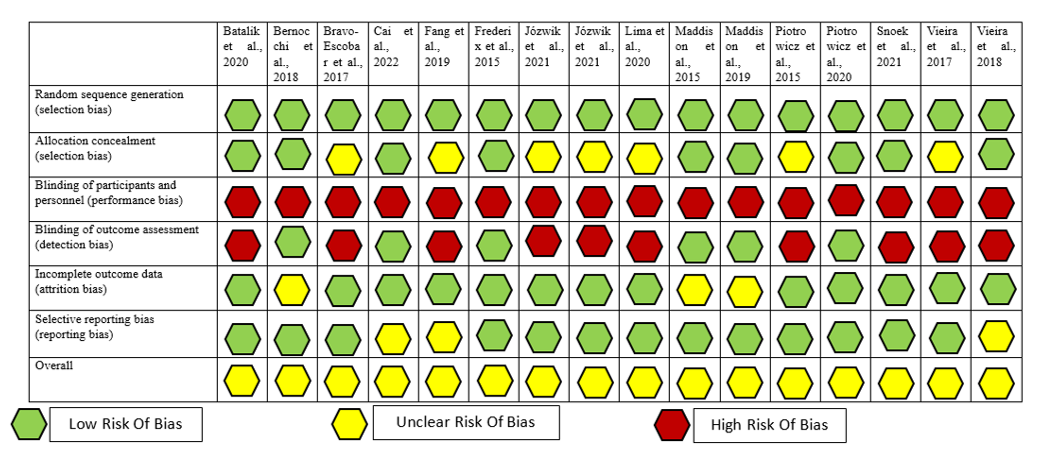
We searched randomized controlled trials (RCTs) in 3 electronic databases: PubMed, Web of Science and Scopus, from January 2015 to January 2024, using relevant keywords. Initially, 502 articles were found, 79 duplicates were identified and eliminated with End Note. All the studies included are evaluated using the Cochrane risk-of-bias tool to assess the risk of all types of bias (selection bias, performance bias, attrition bias, reporting bias, and overall). After that, all the studies were also checked for the Physiotherapy Evidence Database (PEDro) score to perform a quality assessment.
Results
In total, 16 RCTs fulfilled the predefined criteria, which were analysed in our systematic review. Regarding the diseases assessed, 12 studies are about coronary artery diseases (CAD), 1 concerned patients with coexisting chronic obstructive pulmonary disease (COPD) and chronic heart failure (CHF), 1 concerned patients who underwent ablation for atrial fibrillation, 2 concerned patients with Heart Failure (HF).
The technological solutions adopted are the most varied and provide for the detection of vital parameters which are transmitted in real-time by the device which detects them (1-5) or uploaded later by the patients using applications (6-8) in order to allow the safety of the patients during training and the monitoring of the correctness of the rehabilitation programme. Some studies involve only the correct execution of movement by sensor or with the use of virtual reality in CR (9-11) aimed at anxiety and depression management (12, 13) or lung function in post- Coronary Artery Bypass Graft (CABG) patients (14). Finally, in the 2015 study by Maddison et al (16), there is no monitoring system; all outcome measures are based on patient’s self-reported data. In a 2020 study, on the other hand, the same authors use a very comprehensive system that can directly detect and transmit vital and movement parameters (17).
As regards CR programmes, the studies included in our review show a wide range of interventions, based mainly on exercise, sometimes accompanied by patient education on the management of risk factors (dietary interventions, cessation of smoking habits, maintenance of an active lifestyle) and counselling interventions for the management of anxiety and depression. These studies also show a wide range of rehabilitation programme, in terms of types, intensity and duration of exercise training. The rehabilitation programmes mostly focus on exercise and range from a minimum of 6 weeks with a frequency of 3 times per week (27), to a maximum of 24 weeks (34, 35, 39, 40) with a frequency ranging from 3 to 5 times per week. In these studies the exercise type is a moderate-intensity aerobic training (39, 40) alone or combined with strength training and stretching (34, 35). With regard to the studies including the use of virtual reality (36-38) associated with exercise training, there are generally only a few sessions, ranging from 5 to 8, aimed to improve symptoms such as anxiety and depression (36, 37), which are often present in people with CVD, or to enhance the respiratory pattern in post-CABG patients (38). Despite the wide variety of rehabilitation programmes proposed, we report the lack of studies involving exercises to improve flexibility and coordination and only a few studies including respiratory exercises.
As primary outcame, most of the included studies consider Cardiorespiratory fitness (CRF) assessed with Cardiopulmonary exercise testing (CPET), expressed as peak oxygen consumption (VO2 peak) (30-32, 39, 40), maximal oxygen consumption (VO2 max) (41) or as Metabolic Equivalent of Task (MET) (26). Only 2 studies performed a 6-Minute Walking Test (6MWT) to evaluate the possible effects of CTR on the exercise capacity (25, 27). As secondary outcomes in the studies analysed we mostly find assessments of physical activity, Quality of Life (QoL), training adherence, cardiovascular risk factors/laboratory parameters, anxiety and depression level. Physical activity is assessed in different ways, i.e. with the Physical Activity Scale for elderly (PASE) (25), with the International Physical Activity Questionnaire (IPAQ) for the self-reported PA assessment (31, 39, 40) and finally with the use of accelerometry data (33, 41).
Discussion and Conclusion
The aim of this review is to highlight how much telerehabilitation has changed since its beginnings. The technologies used in the included studies show a considerable evolution over time from simpler systems, such as text messages sent via telephone, to more sophisticated platforms, also equipped with virtual reality. Another aim of this review is show what type of rehabilitation program have been mainly used in telerehabilitation and to highlight the effectiveness of telerehabilitation in the treatment of CVD. The rehabilitation treatments used in the included studies are heterogeneous in terms of programme duration, single treatment duration, intensity and type of exercise. In conclusion in this systematic review, we have shown, overall, that CTR can be an advantageous alternative in improving the functional outcome of patients with CVD, especially due to the technological advances we have been assisting in recent years, which allow real-time monitoring and transmission of vital and movement parameters, offering a care experience comparable to traditional center-based rehabilitation. Compared to center-based rehabilitation, moreover, CTR can offer further advantages, with better cost-effectiveness, the breaking down of geographical barriers, and the improvement of access to treatment for the female population, traditionally more socially committed (18). Furthermore, CTR treatment is safe, can lead to increased levels of participation and can improve long-term cardiovascular risk management (19).
REFERENCES
- Bernocchi P, Vitacca M, La Rovere MT, Volterrani M, Galli T, Baratti D, et al. Home-based telerehabilitation in older patients with chronic obstructive pulmonary disease and heart failure: a randomised controlled trial. Age Ageing. 2018;47(1):82-8.
- Bravo-Escobar R, González-Represas A, Gómez-González AM, Montiel-Trujillo A, Aguilar-Jimenez R, Carrasco-Ruíz R, et al. Effectiveness and safety of a home-based cardiac rehabilitation programme of mixed surveillance in patients with ischemic heart disease at moderate cardiovascular risk: A randomised, controlled clinical trial. BMC Cardiovasc Disord. 2017;17(1):66.
- Fang J, Huang B, Xu D, Li J, Au WW. Innovative Application of a Home-Based and Remote Sensing Cardiac Rehabilitation Protocol in Chinese Patients After Percutaneous Coronary Intervention. Telemed J E Health. 2019;25(4):288-93.
- Maddison R, Rawstorn JC, Stewart RAH, Benatar J, Whittaker R, Rolleston A, et al. Effects and costs of real-time cardiac telerehabilitation: randomised controlled non-inferiority trial. Heart. 2019;105(2):122-9.
- Piotrowicz E, Pencina MJ, Opolski G, Zareba W, Banach M, Kowalik I, et al. Effects of a 9-Week Hybrid Comprehensive Telerehabilitation Program on Long-term Outcomes in Patients With Heart Failure: The Telerehabilitation in Heart Failure Patients (TELEREH-HF) Randomized Clinical Trial. JAMA Cardiol. 2020;5(3):300-8.
- Batalik L, Dosbaba F, Hartman M, Batalikova K, Spinar J. Benefits and effectiveness of using a wrist heart rate monitor as a telerehabilitation device in cardiac patients: A randomized controlled trial. Medicine (Baltimore). 2020;99(11):e19556.
- Cai C, Bao ZP, Wu N, Wu FM, Sun GZ, Yang G, et al. A novel model of home-based, patient-tailored and mobile application-guided cardiac telerehabilitation in patients with atrial fibrillation: A randomised controlled trial. CLINICAL REHABILITATION. 2022;36(1):40-50.
- Piotrowicz E, Zieliński T, Bodalski R, Rywik T, Dobraszkiewicz-Wasilewska B, Sobieszczańska-Małek M, et al. Home-based telemonitored Nordic walking training is well accepted, safe, effective and has high adherence among heart failure patients, including those with cardiovascular implantable electronic devices: a randomised controlled study. Eur J Prev Cardiol. 2015;22(11):1368-77.
- Frederix I, Hansen D, Coninx K, Vandervoort P, Vandijck D, Hens N, et al. Effect of comprehensive cardiac telerehabilitation on one-year cardiovascular rehospitalization rate, medical costs and quality of life: A cost-effectiveness analysis. Eur J Prev Cardiol. 2016;23(7):674-82.
- Vieira ASD, de Melo M, Pinho A, Machado JP, Mendes JGM. The effect of virtual reality on a home-based cardiac rehabilitation program on body composition, lipid profile and eating patterns: A randomized controlled trial.
- Vieira A, Melo C, Machado J, Gabriel J. Virtual reality exercise on a home-based phase III cardiac rehabilitation program, effect on executive function, quality of life and depression, anxiety and stress: a randomized controlled trial. DISABILITY AND REHABILITATION-ASSISTIVE TECHNOLOGY. 2018;13(2):112-23.
- Józwik S, Cieslik B, Gajda R, Szczepanska-Gieracha J. Evaluation of the Impact of Virtual Reality-Enhanced Cardiac Rehabilitation on Depressive and Anxiety Symptoms in Patients with Coronary Artery Disease: A Randomised Controlled Trial. JOURNAL OF CLINICAL MEDICINE. 2021;10(10).
- Józwik S, Cieslik B, Gajda R, Szczepanska-Gieracha J. The Use of Virtual Therapy in Cardiac Rehabilitation of Female Patients with Heart Disease. MEDICINA-LITHUANIA. 2021;57(8).
- Lima HD, Souza RDP, Santos A, Borges DL, Guimaraes ARF, Ferreira G, et al. Virtual reality on pulmonary function and functional independence after coronary artery bypass grafting: clinical trial. AMERICAN JOURNAL OF CARDIOVASCULAR DISEASE. 2020;10(4):499-505.
- Maddison R, Pfaeffli L, Whittaker R, Stewart R, Kerr A, Jiang Y, et al. A mobile phone intervention increases physical activity in people with cardiovascular disease: Results from the HEART randomized controlled trial. Eur J Prev Cardiol. 2015;22(6):701-9.
- Maddison R, Rawstorn JC, Stewart RAH, Benatar J, Whittaker R, Rolleston A, et al. Effects and costs of real-time cardiac telerehabilitation: randomised controlled non-inferiority trial. HEART. 2019;105(2):122-9.
- Snoek JA, Meindersma EP, Prins LF, van’t hof AWJ, de Boer MJ, Hopman MT, et al. The sustained effects of extending cardiac rehabilitation with a six-month telemonitoring and telecoaching programme on fitness, quality of life, cardiovascular risk factors and care utilisation in CAD patients: The TeleCaRe study. JOURNAL OF TELEMEDICINE AND TELECARE. 2021;27(8):473-83.
- Brouwers RWM, van Exel HJ, van Hal JMC, Jorstad HT, de Kluiver EP, Kraaijenhagen RA, et al. Cardiac telerehabilitation as an alternative to centre-based cardiac rehabilitation. Neth Heart J. 2020;28(9):443-51.
- Zhong W, Liu R, Cheng H, Xu L, Wang L, He C, et al. Longer-Term Effects of Cardiac Telerehabilitation on Patients With Coronary Artery Disease: Systematic Review and Meta-Analysis. JMIR Mhealth Uhealth. 2023;11:e46359.