Pregnolato Giorgia [Healthcare Innovation Technology Lab, San Camillo IRCCS Hospital, Venice, Italy]
Severini Giacomo [School of Electrical and Electronic Engineering, University College Dublin, Dublin 4, Dublin, Ireland]
Privitera Luigi [The BioRobotics Institute, Scuola Superiore Sant’Anna and the Department of Excellence in Robotics and AI, Scuola Superiore Sant’Anna, Italy]
Ariano Paolo [Morecognition Ltd, Turin, Italy]
Turolla Andrea [Department of Biomedical and Neuromotor Sciences — DIBINEM, Alma Mater Studiorum Università di Bologna, Via Massarenti, 9, 40138 Bologna, Italy]
Picelli Alessandro [Department of Neurosciences, Biomedicine and Movement Sciences, University of Verona, 37100 Verona, Italy]
In the investigation of the neural mechanisms underlying voluntary movements, the muscle synergies model has gained considerable traction. Muscle synergies are described as a set of muscles activated with a defined contribution and recruited with variable intensity and timing[1]. Muscle synergies are extracted applying decomposition algorithms from surface electromyography (sEMG) signals recorded during tasks execution[2]. In stroke rehabilitation, the implementation of muscle synergies analysis in clinical assessment has enabled the quantification of motor impairment and the prediction of motor recovery[3]. While many acquisition protocols have been implemented for upper limb assessment, there is still a need for one for hand assessment[4]. This is due to the variability among the subjects and the instrumental methods used [4]. In this PhD project, the main goal was to investigate the muscle synergies model to describe motor recovery at both upper limb (Study 1) and hand motor functions (Study 2), after stroke.
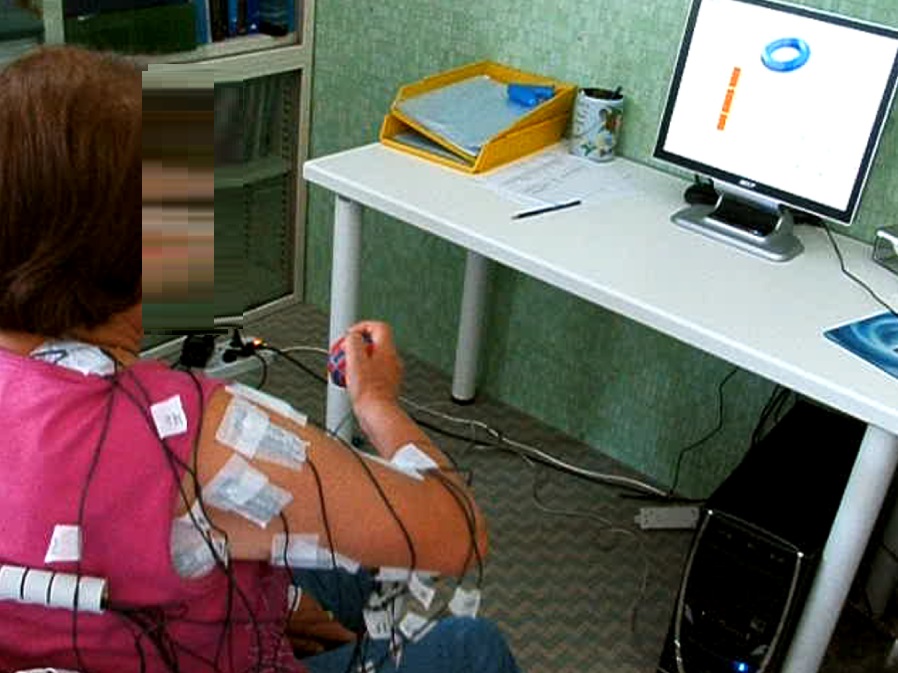
In Study 1, we analysed muscle synergies parameters of the upper limb (i.e. number of modules, percentage of merged muscle synergies) extracted from sEMG recorded by 16 muscles, both in affected and unaffected upper limbs. We collected data from 62 stroke survivors, who underwent a specific upper limb motor treatment (1h/day, 5times/week, 20 sessions).
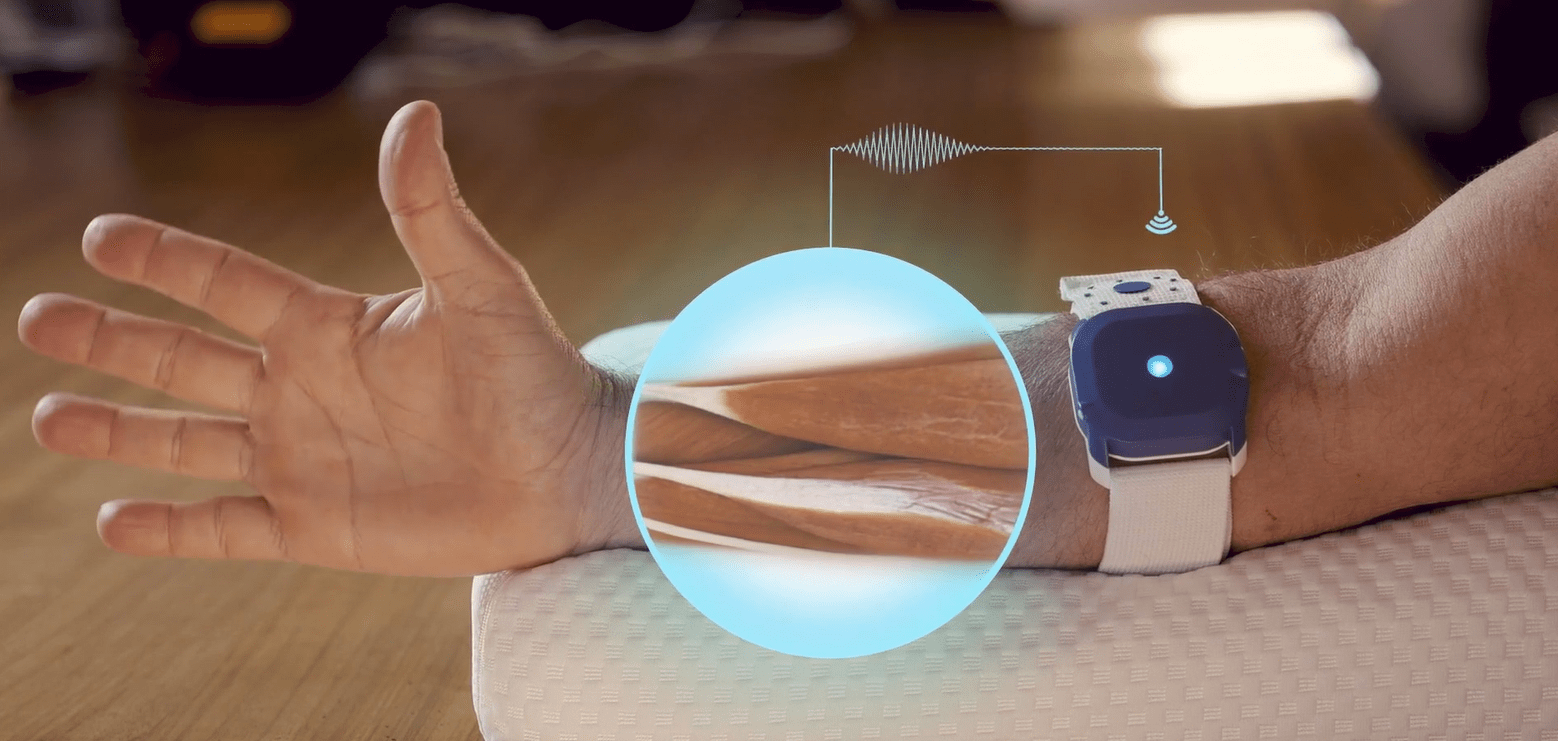
In Study 2, we developed a wearable device REMO for hand therapeutic application (Morecognition Ltd, Turin, Italy), composed by 8 dry bipolar sEMG electrodes able to detect muscles activation during hand movements. First, we certified REMO as Class1 medical device, then we defined the clinical features needed to control 1, 5 or 10 gestures using REMO, in a rehabilitation setting, in people with stroke. Finally, we implemented a new muscle-synergies-based index to describe muscle activation similarity between 4 healthy subjects and 10 people with stroke, following a hand specific motor training (1h/day, 5times/week, 15 sessions).
In Study 1, overall patients improved upper limb motor function (mean improvement at Fugl-Meyer Assessment-Upper Extremity, FMA-UE=7.2±7.5; p<0.001), but not the number of muscle synergies extracted from the affected limb (mean difference=-0.2±1.1; p=0.374). According to the Minimally Clinically Important Difference of FMA-UE (Δ > 5 points), 34 patients responded to treatment (Responder) and 28 did not (Non-Responder). Only the percentage of merged muscle synergies differed between groups, with the Responder group significantly decreased (Δ Responder=-12.2%; Δ Non-Responder =1.8%; p=0.004).
In Study 2, the use of REMO in people with stroke was predicted by mild impairment of upper limb function (FMA-UE > 18 points), no spasticity at flexor carpii muscle, no pain, neither joint restriction. Overall, patients showed recovery of hand function (mean improvement at FMA-hand= 3.6±1.9; p< 0.001) and improved sEMG similarity index only in pinch grasp (mean difference= 7.2±13.5; p< 0.001).
In conclusion, muscle synergies analysis may provide new information on neural mechanisms underpinning recovery of upper limb and hand motor function. Upper limb rehabilitation therapies induced reduction of muscle synergies merging in people with stroke, in according to clinically important improvement of motor function (i.e., Responder patients). As for hand rehabilitation, the information provided by similarity index is not yet fully coherent with clinical outcome measures. Thus, advancements of protocols for muscle synergies extraction and calculation of similarity index are needed to improve assessment performance of upper limb and hand motor function, by wearable devices like REMO.
[1] Bizzi E, Mussa-Ivaldi FA, Giszter S. Computations underlying the execution of movement: a biological perspective. Science. 1991 Jul 19;253(5017):287-91. doi: 10.1126/science.1857964. PMID: 1857964.
[2] D’Avella A, Saltiel P, Bizzi E. Combinations of muscle synergies in the construction of a natural motor behavior. Nat Neurosci. 2003 Mar;6(3):300-8. doi: 10.1038/nn1010. PMID: 12563264.
[3] Cheung VC, Turolla A, Agostini M, Silvoni S, Bennis C, Kasi P, Paganoni S, Bonato P, Bizzi E. Muscle synergy patterns as physiological markers of motor cortical damage. Proc Natl Acad Sci U S A. 2012 Sep 4;109(36):14652-6. doi: 10.1073/pnas.1212056109. Epub 2012 Aug 20. PMID: 22908288; PMCID: PMC3437897.
[4] Zhao K, Zhang Z, Wen H, Liu B, Li J, Andrea d’Avella, Scano A. Muscle synergies for evaluating upper limb in clinical applications: A systematic review. Heliyon. 2023 May 11;9(5):e16202. doi: 10.1016/j.heliyon.2023.e16202. PMID: 37215841; PMCID: PMC10199229.