Come standardizzare i fattori di rischio per le cadute in ospedale? Un nuovo approccio multifase attraverso un proof-of-concept study
How to standardize reported risk factors for falls in hospital? A new multi-phase approach using a proof-of-concept study
Autori
Caselli Serena [Unità Operativa Complessa di Medicina Riabilitativa, Azienda Ospedaliero-Universitaria di Modena, Modena, Italy]
La Porta Fabio [IRCCS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italy]
Valpiani Giorgia [Research and Innovation Unit, Biostatistics and Clinical Trial Area, University Hospital of Ferrara, Ferrara, Italy]
Lullini Giada [IRCCS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italy]
Negro Antonella [Innovation in Healthcare and Social Services, Emilia-Romagna Region, Bologna, Emilia-Romagna, Italy]
Pellicciari Leonardo [IRCCS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italy]
Bassi Erika [Department of Translational Medicine, University of Eastern Piedmont, Novara, Italy]
Pecoraro Valentina [Department of Laboratory Medicine and Pathology, AUSL Modena, Modena, Italy]
Govoni Erika [[Innovation in Healthcare and Social Services, Emilia-Romagna Region, Bologna, Emilia-Romagna, Italy – Unità Organizzativa Riabilitazione Ospedaliera, Dipartimento Assistenziale Tecnico e Riabilitativo, Ausl Bologna, Bologna, Italy]
Introduction
In-hospital falls are a public health issue resulting in enormous individual, social and health costs. To prevent in-hospital falls, it is essential to know the risk factors (RFs) so that they can be recognized and prevented or modified through clinical interventions. The literature reports uncertainty and inconsistency in RF terminology for in-hospital falls that could be reduced by linking RFs to standardized health concepts, such as those provided by the conceptual categories of the WHO International Health Classifications. Therefore, this study, conducted by Innovation in Healthcare and Social Services of Emilia-Romagna Region, aims: 1) to perform a literature review to identify fall RFs among hospitalized adults; 2) to link the found RFs to the corresponding health classification categories to reduce the heterogeneity of their definitions; 3) to perform a meta-analysis on risk categories to identify significant RFs; and 4) to refine the definitive list of significant categories to avoid redundancies.
Methods
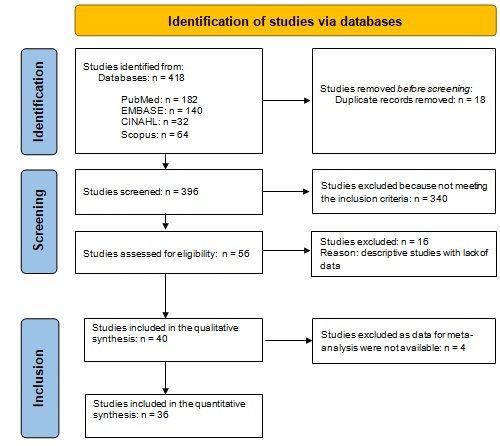
The review protocol was registered prospectively on the PROSPERO register (CRD42022328922). Four databases were queried. We included observational studies assessing patients who had experienced in-hospital falls, published in English or Italian until March 2022. Two independent reviewers performed the inclusion and extrapolation process. They evaluated the methodological quality (using National Institute of Health (NIH) quality assessment tools for case-control studies and observational cohort and cross-sectional studies) of the included studies. RF records were linked to the categories of three health classifications (International Classification of Functioning, Disability, and Health [ICF], International Classification of Diseases version 10 [ICD-10], Anatomical Therapeutic Chemical Classification [ATC]). Meta-analyses were performed to obtain an overall pooled odds ratio (OR) for each category, which aggregated single RFs, using a random effect model. Finally, significant RF categories were considered after the exclusion of redundant RFs across different classifications.
Results
Thirty-six articles were included in the meta-analysis. 1,111 RF records were identified; 616 were linked to ICF classification, 450 to ICD-10, and 260 to ATC. Considering the ICF, the meta-analysis identified 50 RF categories linked to 523 records as significant (52 RFs non-significant). Regarding ICD-10, the meta-analysis identified 51 RF categories for a total of 509 records as significant (101 RFs non-significant). Concerning ATC, the meta-analysis identified 26 RF categories linked to 294 records as significant (65 RFs non-significant). 18 RF categories were excluded as they were redundant or protective factors. After this process, the purified list included 53 significant RF categories linked to 328 records. The pooled OR values of the purified list ranged from 1.299 (N06A Antidepressants) to 8.633 (d420 Transferring oneself). Overall, the initial number of RFs was reduced by about 21 times compared to the initial number, i.e., from 1,111 identified RF records to 53 significant RF categories.
Discussion and Conclusion
This study aimed to provide a proof-of-concept that it may be feasible to reduce the reported heterogeneity in the description of fall RFs and, subsequently, their number by adopting the standard terminology provided by the International Health Classifications. We achieved this aim in four subsequent steps, and we identified 53 significant RF categories for in-hospital falls. We demonstrated that adopting a clear and consistent terminology derived from standardized international classifications may lead to a marked reduction and systematization of fall RFs among hospitalized adults. The list of significant RFs can be used as a template at the regional level to build more accurate measurement instruments to predict in-hospital falls.
REFERENCES
Deandrea, S, Bravi, F, Turati, F, Lucenteforte, E, La Vecchia, C, and Negri, E. Risk factors for falls in older people in nursing homes and hospitals. A systematic review and meta-analysis. Arch Gerontol Geriatr. (2013) 56:407–15. doi: 10.1016/j.archger.2012.12.006
Cieza, A, Fayed, N, Bickenbach, J, and Prodinger, B. Refinements of the ICF linking rules to strengthen their potential for establishing comparability of health information. Disabil Rehabil. (2019) 41:574–83. doi: 10.3109/09638288.2016.1145258