Muscle co-contraction activity in altered visual perception of the hand: a case report on a stroke patient in virtual rehabilitation-guided reaching and grasping tasks
Autori
Pagano Alessandro [Department of Experimental and Clinical Medicine – University Politecnica delle Marche, Ancona, Italy]
Tigrini Andrea [Department of Information Engineering – Università Politecnica delle Marche, Ancona, Italy]
Bonci Viviana [Department of Experimental and Clinical Medicine – Università Politecnica delle Marche, Ancona, Italy]
Capriotti Alessandro [Department of Mental and Physical Health – Unicampania, Naples, Italy]
Ceravolo Maria Gabriella [Department of Experimental and Clinical Medicine – Università Politecnica delle Marche, Ancona, Italy]
Burattini Laura [Department of Information Engineering – Università Politecnica delle Marche, Ancona, Italy]
Capecci Marianna [Department of Experimental and Clinical Medicine – Università Politecnica delle Marche, Ancona, Italy]
Introduction to clinical case
Visuomotor adaptation (VMA) is a form of motor learning that enables individuals to adjust their movements in response to visual distortions [1]. This adaptive process is often compromised in post-stroke patients due to motor and sensory deficits, including abnormal co-contraction of agonist and antagonist muscles and altered body representation. Immersive virtual reality (VR) offers new possibilities to study and promote neuroplasticity, with promising effects on motor control and VMA [2]. However, no studies have yet examined how VR-induced modifications of internal body representation affect VMA. This study investigates whether visually altering hand size in a virtual environment can influence VMA, potentially informing new strategies for motor rehabilitation in stroke survivors.
Methods
Surface electromyographic (sEMG) activity was recorded using the FREEEMG system (BTS Bioengineering) from eight upper limb muscles: adductor pollicis (AP), flexor and extensor carpi radialis (FC, EC), finger extensor (ED), biceps brachii (BB), triceps brachii (TB), anterior deltoid (DA), and upper trapezius (TS). Participants performed reaching and grasping tasks in a virtual environment while viewing a visual representation of their hand with either enlarged or reduced dimensions. The same tasks were repeated in two control conditions: a real-world setting and a virtual environment with no hand-size alteration. EMG signals were band-pass filtered (20–450 Hz), rectified, and envelope-extracted. An on–off detection algorithm was used to segment EMG activity across repetitions [3]. The co-contraction index (CCI) [4] was calculated for each agonist-antagonist muscle pair. Statistical comparisons between conditions (modified hand-size vs normal size) were made using the Wilcoxon rank-sum test (p < 0.05).
Results
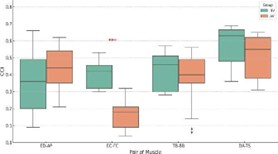
A significant difference was observed for the EC–FC muscle pair, with a lower CCI found during tasks involving altered hand size (median 0.18) compared to tasks with normal hand size (0.42, p < 10⁻⁴). Although not statistically significant, consistent decreases in CCI were also observed for the DA–TS (0.55 vs. 0.63) and TB–BB (0.40 vs. 0.46) pairs under altered visual conditions. Interestingly, the ED–AP pair was the only case showing a higher median CCI in the altered hand size condition (0.44) compared to the normal one (0.36), though this difference also did not reach statistical significance (p > 0.05).
Discussion and clinical relevance
These preliminary findings suggest that altered visual feedback in VR may reduce pathological muscle co-contraction, promoting more efficient and synergistic movements. Further research on larger post-stroke populations is needed to confirm these effects and explore their clinical potential.
REFERENCES
[1] E. Tzvi, S. Loens, et al. Cerebellum. (2022): 306–313
[2] F. Amin, A. Waris et al. IEEE Trans Neural Syst Rehabil Eng. (2024): 32:2060-2069
[3] Rashid, Usman, et al. Journal of Electromyography and Kinesiology 48 (2019): 103-111.
[4] Unnithan, V. B., et al. Electromyography and clinical neurophysiology 36.8 (1996): 487-494.