THE CLINICAL RESULTS OF COMBINATION OF ANXIOLYSIS, SUPRASCAPULAR NERVE BLOCK, CORTICOSTEROID INJECTION AND PHYSIOTHERAPY ON SUBJECTS WITH FROZEN SHOULDER: A RETROSPECTIVE STUDY
Autori
Martino Gabriele (University of Molise, Campobasso, Italy)
Venturin Davide (University of Molise, Campobasso, Italy)
Pellicciari Leonardo (IRCCS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italy)
Casagrande Lucia (Azienda ULSS 2, Marca trevigiana, Treviso, Italy)
Brindisino Fabrizio (University of Molise, Campobasso, Italy)
Poser Antonio (University of Siena, Siena, Italy)
Background and aims
Frozen shoulder (FS) is a gleno-humeral pathology characterized by an insidious onset, increasing pain and loss of active and passive range of motion. The restriction of mobility is related to modification of collagen, overexpression of proteins and to presence of muscle guarding. The presence of muscle guarding and pain could reduce the efficacy of the physiotherapy, the adherence to the treatment and could increase emotional commitment during rehabilitation. The aim of this study was to evaluate the clinical results of a combined treatment of anxiolysis and SupraScapular Nerve Block (SSNB) with intra-articular corticosteroid injection and physiotherapy in subjects with FS.
Methods
29 subjects received SSNB, intra-articular corticosteroid injections, and intravenous anxiolysis, followed 30 minutes later by physiotherapy involving end-range, high-grade, and painful glenohumeral mobilizations, repeated throughout the first month. Participants were also instructed to perform 5 home stretching exercises for three months. Outcomes—pROM, SF-36 (and subscores), DASH, and SPADI—were assessed at baseline (T0), day 10 (T1), and 3-month follow-up (T5).
Results
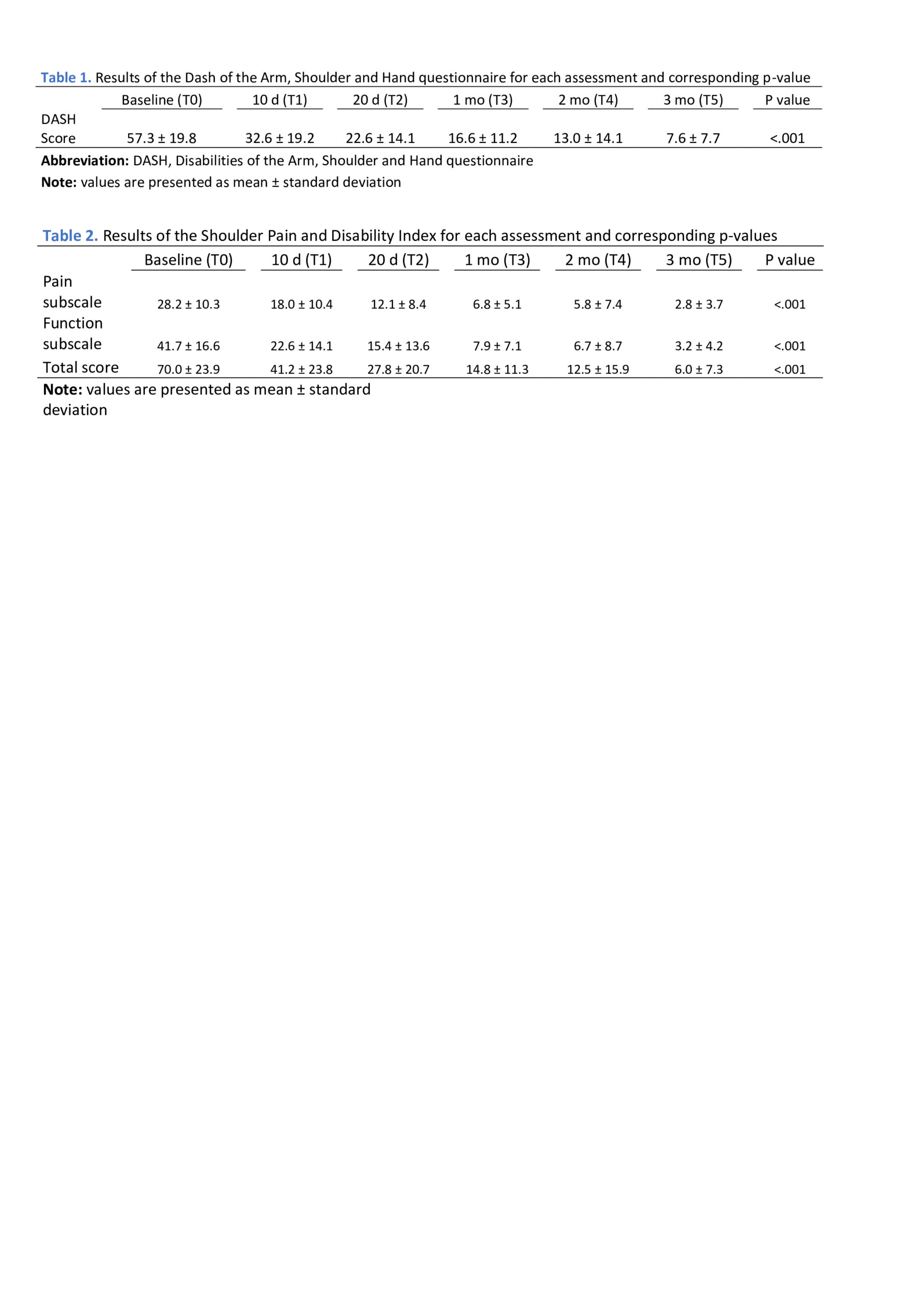
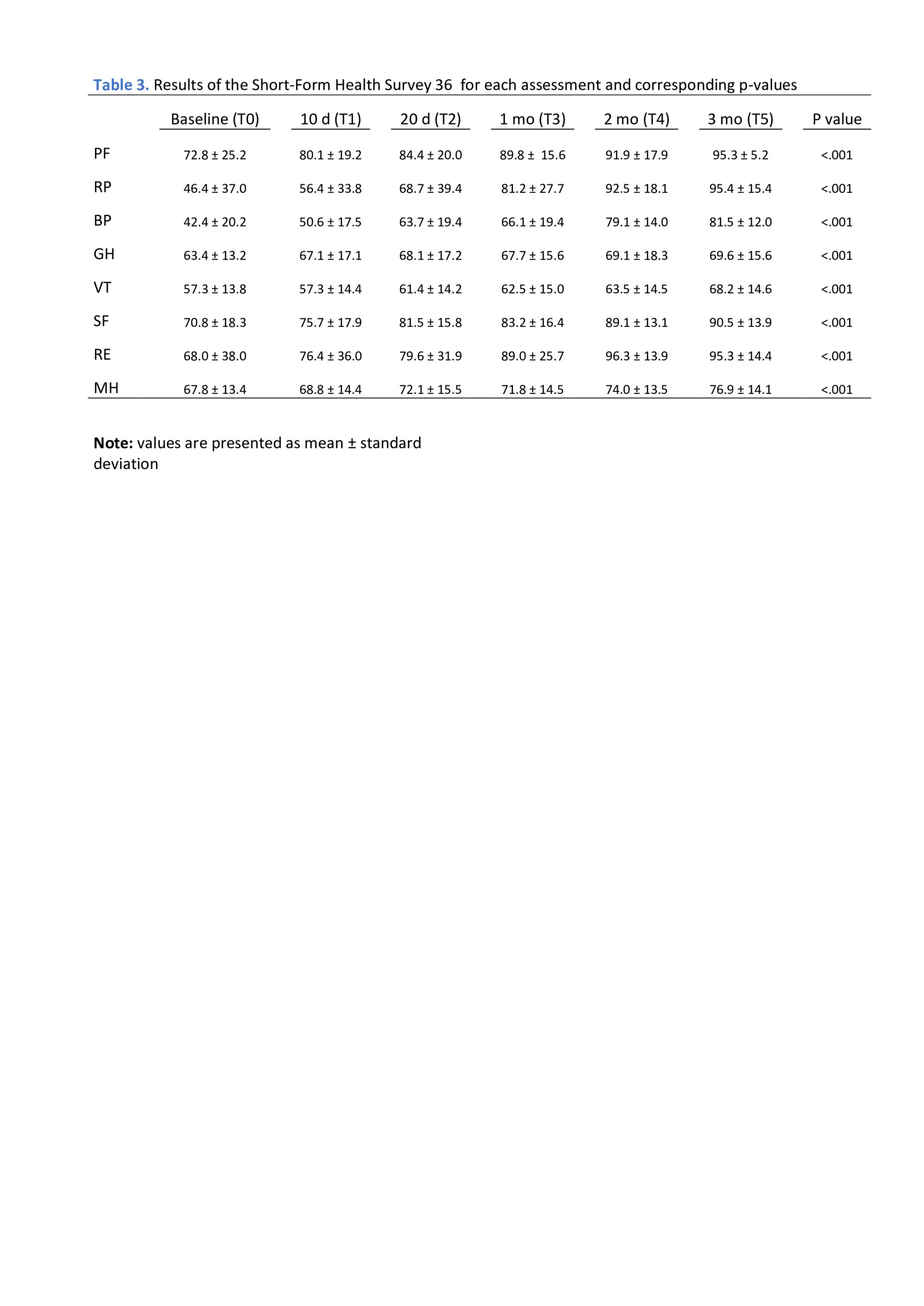
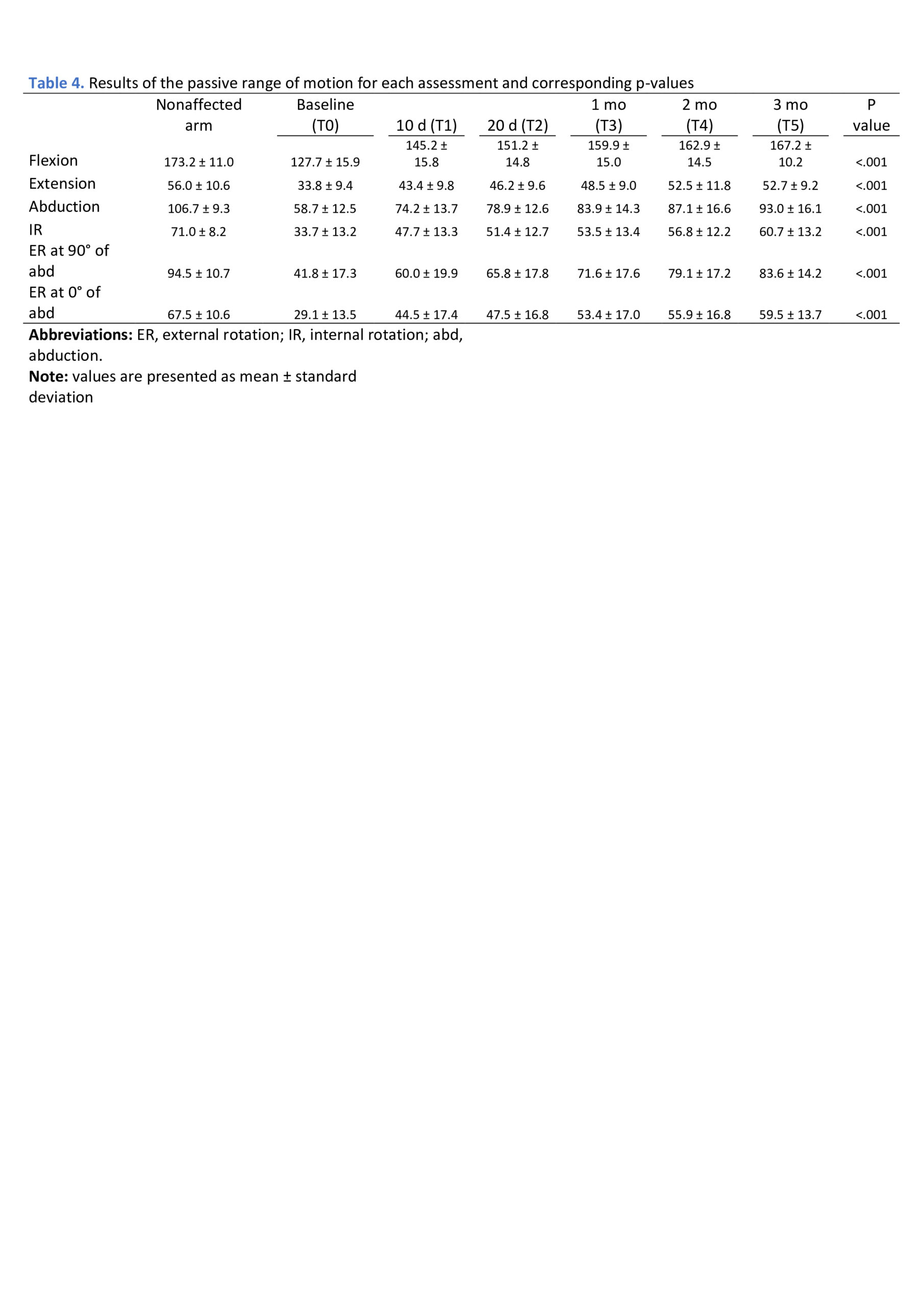
SPADI and DASH scores showed significant improvement from T1 (p = .000), maintained through T5 (Table 1-2). SF-36 subscales for Physical Functioning, Physical Role, and Emotional Role reached statistical significance at T3 (p = .007; .000; .034), T4 (.001; .000; .003), and T5 (.001; .000; .004). Bodily Pain and Social Functioning showed improvements from T2 (p = .003; .043) through T5 (.000; .000). Vitality and Mental Health were significant at T4 (.017; .007) and T5 (.000; .001) (Table 3). All average pROM scores improved significantly from T1 to T5, with clinically relevant gains in flexion, abduction, and external rotation at both 90° and 0° of abduction compared to T0 (Table 4).
Conclusion
The combination of anxiolysis, injection and SSNB could have been useful to create a therapeutic window in the first session, during which painful mobilization and stretching techniques could be applied more successfully and to allow a quicker recovery in the short term, orienting through a multi-professional path of care would be helpful for subjects with FS. Anxiolysis, SSNB, and intra-articular corticosteroid injections, combined with a detailed rehabilitation techniques and a simple home exercise program, were effective in improving shoulder pain, range of motion, and disability in the short term.
REFERENCES
1- Lewis J. Frozen shoulder contracture syndrome – Aetiology, diagnosis and management. Man Ther. 2015
Feb 1;20(1):2–9.
2- Hollmann L, Halaki M, Kamper SJ, Haber M, Ginn KA. Does muscle guarding play a role in range of motion loss in patients with frozenshoulder? Musculoskelet Sci Pract. 2018 Oct 1;37:64–68.
3- Venturin D, Brindisino F, Ristori D, et al. The use of corticosteroid/anesthetic injections in conjunction with physical therapy in the treatment of idiopathic frozen shoulder: a case series. JOSPT Cases. 2021;1(4):248–265.