The Early Functional Abilities-revised may bridge the measurement gap between the disorder of consciousness and the functional independence scales: a Rasch analysis study
Introduction
A measurement gap between the disorder of consciousness (DoC) and functional independence scales is present, as both cannot measure the recovery of early functional changes occurring on emergence from DoC. The Early Functional Abilities scale (EFA) was developed to bridge this gap. It describes clinically observable changes concerning purposeful activities, illness and disability awareness, and the ability to comply with medical, nursing, and therapeutic interventions.
In 2018, Poulsen et al. assessed the internal construct validity (ICV), reliability, and measurement precision of EFA in patients with TBI with Rasch analysis. The analysis rejected unidimensionality and did not recommend summarizing the four subscale measures into an EFA total score.
This study investigated whether selecting a valid content subset of items (EFA-R) from the original EFA was possible, providing an essentially unidimensional measurement of early functional ability.
Methods
In a multicenter observational cross-sectional study, we included three hundred sixty-two adults diagnosed with DoC due to a severe acquired brain injury (sABI) on admission to eleven Italian rehabilitation centers. We excluded patients with pre-existing neurological degenerative pathologies and/or concurrent illnesses likely to compromise survival within six months. Each patient was represented with only one chosen random evaluation in the dataset to avoid the risk of time dependency.
The Italian version of EFA (20 items with a five-point score grouped in 4 subscales) was administered to the sample and then submitted to Mokken analysis (MA), Confirmatory Factor Analysis (CFA), Rasch analysis, Confirmatory Bifactor Analysis (CBA), and external construct validity.
When available, we also collected the Coma Recovery Scale-Revised (CRS-R) and the FIMTM for each person at the same time point for sample description and external validity purposes.
Results
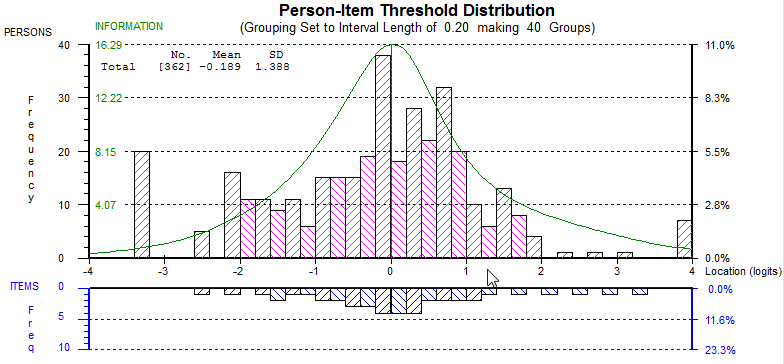
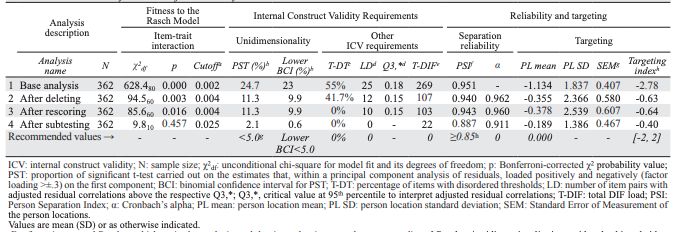
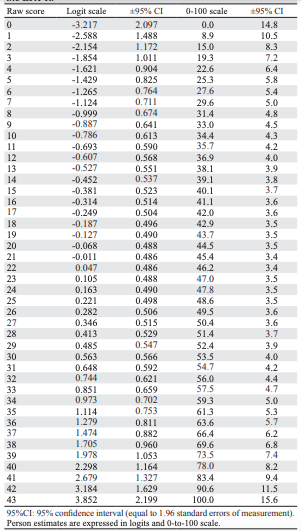
According to MA and CFA, the Italian EFA showed sufficient preliminary unidimensionality. Within Rasch Analysis, a final 12-item solution (EFA-R) was calibrated. EFA-R is “essentially unidimensional” according to 1) analysis of residual correlations supporting item essential local independence; 2) a robust correlation between item subtests (rho=0.950); 3) only 2.1% of cases with significant difference between person parameter estimates by different subscales; 4) an explained common variance equal to 0.916 obtained from a final CBA. The invariance requirement (unconditional χ2df=9.8120; p=0.457, conditional class-interval based χ2df=33.135; P=0.557) and monotonicity were also satisfied (Table 1). The reliability (Person Separation Index=0.887) was adequate for person measurements (Figure 1). A practical raw-score-to-measure conversion table based on the EFA-R calibration was devised (Table 2). Finally, EFA-R strongly correlated with CRS-R (rho=0.922) and motor FIM™ (rho=0.808).
Discussion and Conclusion
EFA-R is an essentially unidimensional subset of 12 items with adequate ICV and sufficient reliability for individual measurement under the Rasch Model Theory framework in patients with sABI. It has the potential to measure people’s functional abilities whose consciousness is improving despite ongoing severe motor-functional impairments during the early stages of rehabilitation. It covers all four original conceptual domains. The item hierarchy was consistent with the theoretical and expected order of functional recovery in these patients. The raw-score-to-measure conversion table provides interval-level estimates of early functional abilities, essential for correctly interpreting change scores and using parametric statistics.
Given the strong correlation with CRS-R and mFIMTM, it provides “a measurement bridge” between the DoC and the functional independence scales in patients with sABI, overcoming the ceiling and floor effects of the two scales (Figure 2).
REFERENCES
- Heck G, Steiger-Bächler G, Schmidt T. Early Functional Abilities (EFA) – eine Skala zur Evaluation von Behandlungsverläufen in der neurologischen Frührehabilitation. Neurol Rehabil 2000;6:125–33.
- Poulsen I, Kreiner S, Engberg AW. Validation of the Early Functional Abilities scale: an assessment of four dimensions in early recovery after traumatic brain injury. J Rehabil Med 2018;50:165–72.
- Tennant A, Conaghan PG. The Rasch measurement model in rheumatology: what is it and why use it? When should it be applied, and what should one look for in a Rasch paper? Arthritis Rheum 2007;57:1358–62.
- La Porta F, Caselli S, Ianes AB, Cameli O, Lino M, Piperno R, et al. Can we scientifically and reliably measure the level of consciousness in vegetative and minimally conscious States? Rasch analysis of the coma recovery scale-revised. Arch Phys Med Rehabil 2013;94:527– 535.e1.