Proposal of two percentage indices to measure overall joint mobility and segmental mobility useful for managerial purposes
Introduction
Outcome measures used in physiotherapy are typically intended and validated for a particular disease, joint or setting [ 1 ]. For clinical purposes, this is the correct approach. However, functional recovery cannot be compared between different anatomical districts or among different diseases. Such a comparison would be extremely useful at the management level to monitor the overall effectiveness of the physiotherapy interventions.
To address this issue, we developed and tested two indices of joint mobility and segmental mobility that can be used for all joints and with a 0-100 scoring system. Joint mobility depends on the anatomical structural constraints of the joint. Segmental mobility is also affected by other non-anatomical variables, such as pain and muscle strength.
Methods
The joint mobility index (JMI) was computed for each joint as follows: 1) the ROM measurement methodology was standardized according to available literature [ 2 ]; 2) joint maximum excursion in each direction was measured and expressed as a percentage of its normative reference value [ 2 ], leading to a 0-100 grading; and 3) the mean value among all possible joint movements (e.g., flexion, extension, abduction, etc.) was computed. JMI was computed for the following joints: shoulder, elbow, wrist, hip, knee, and ankle (non-axial joints).
With the same approach, the segmental mobility index (SMI) was also computed. This is a multi-dimensional index that takes into account JMI (as computed above), pain at rest, pain during movement, and strength. Pain was assessed using the verbal numeric rating scale [ 3 ]. Muscle strength was measured with the appropriate Manual Muscle Test. Variables were expressed as a percentage of the corresponding normative value and averaged to produce SMI.
Results
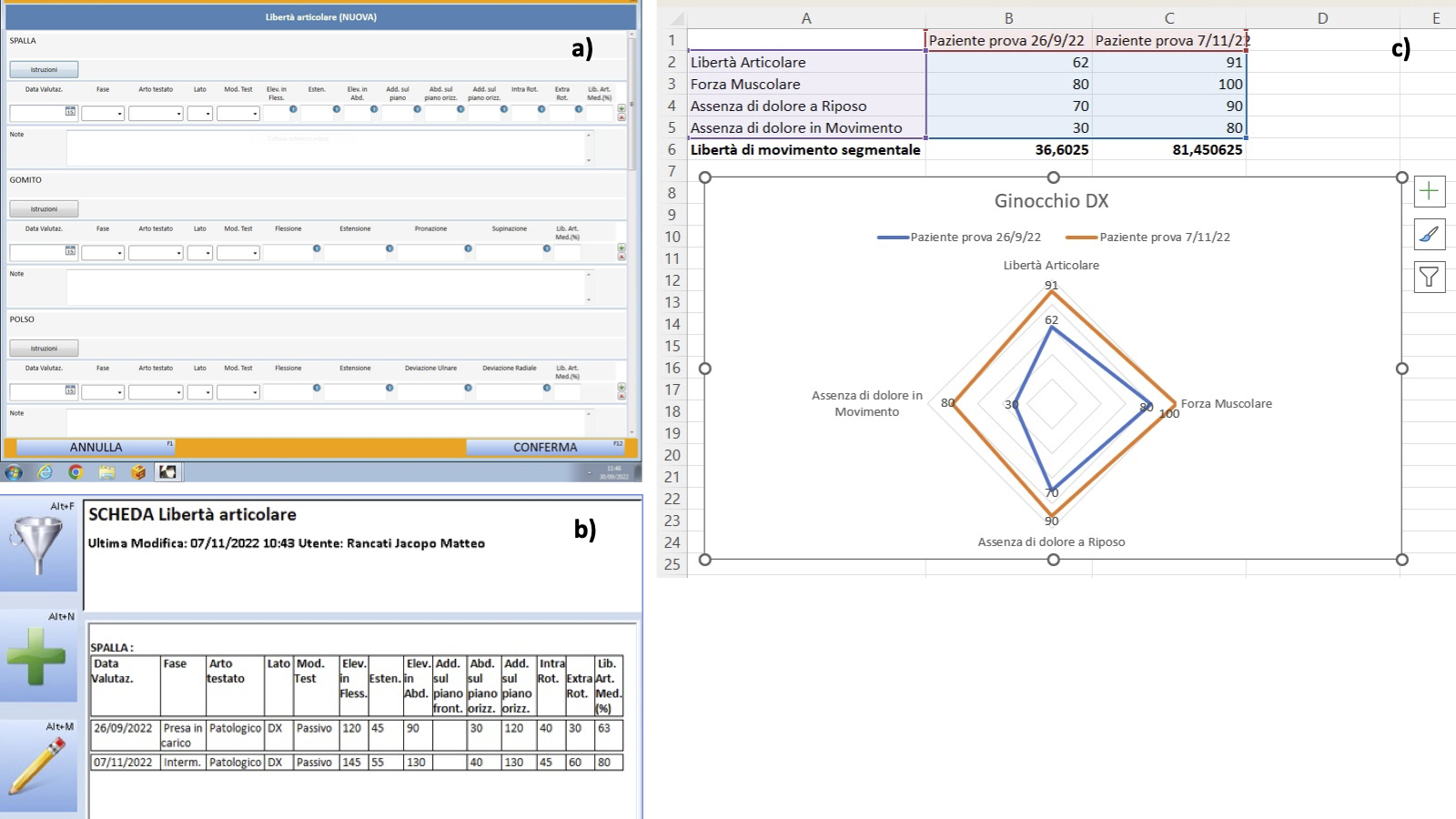
A form for JMI computation has been created and added to the electronic medical record of our institution. (Figure 1a). It allows for JMI computation for both the affected and contralateral side (when needed), during active and passive movements, and in subsequent assessment (e.g., admission, hospital stay, discharge). An example of its use is presented for the shoulder joint in Figure 1b, where the increase in SMI (last column) can be seen. An example of the use of SMI is presented in Figure 1c. The increase in both numerical values and plot area is clearly visible.
Discussion and Conclusion
We developed two indices that can be used to follow the recovery in joint mobility and segmental mobility in patients with different diseases and in different settings. Their feasibility and usefulness are currently under test at our institution.
ROM measurements and clinical scales remain key in clinical practice and at the single-patient level. The two proposed indices, one unidimensional and one multidimensional, could be useful at the organizational and managerial level thus providing a broad overview of patients’ recovery following physiotherapy interventions in a ward, a unit, or a hospital.
Further improvements can be added to the current indices, such as the use of age- and gender-matched normative values and the inclusion of other disorders that could hinder segmental mobility (e.g., lymphedema, scar tissue complications, etc.).
REFERENCES
- Haigh R, Tennant A, Biering-Sørensen F, Grimby G, Marincek C, Phillips S, Ring H, Tesio L, Thonnard JL. The use of outcome measures in physical medicine and rehabilitation within Europe. J Rehabil Med. Novembre 2001; 33(6):273-8.
- Clarkson HM, Gilewich GB. Valutazione cinesiologica. Esame della mobilità articolare e della forza muscolare. 2° Ed. Milano: Edi.Ermes; 2002. 432 p.