Implementation of a Lymphedema Counseling Service in Reggio Emilia: An Integrated Organizational Model within the Territorial Lymphedema Network
Autori
Dimatteo Mariangela (FT) – Medicina fisica e riabilitazione ASMN, AUSL-IRCCS di Reggio Emilia – Italia; Studente del master in Riabilitazione in linfologia clinica Universitaria La Sapienza di Roma
Alice Pecorari (FT) Servizio RRF di Correggio, AUSL-IRCCS di Reggio Emilia, Italia; Studente del master in Riabilitazione in linfologia clinica Universitaria La Sapienza di Roma
Bassoli Agnese (FT) Servizio NPIA, AUSL-IRCCS di Reggio Emilia, Italia; Laureanda magistrale in scienze riabilitative delle professioni sanitarie presso Univr – Università degli studi di Verona
Piccinelli Barbara (Medico Fisiatra) Medicina fisica e riabilitazione ASMN, AUSL-IRCCS di Reggio Emilia, Italia
Manfredi Nicoletta (FT) Medicina fisica e riabilitazione ASMN, AUSL-IRCCS di Reggio Emilia, Italia
Giberti Tiziana (FT) Servizio RRF CNM, AUSL-IRCCS di Reggio Emilia, Italia
Isabella Campanini, PhD LAM (Dip. Neuromotorio Riabilitativo) AUSL-IRCCS di Reggio Emilia
Rancati Jacopo Matteo (Dirigente Professioni Sanitarie della Riabilitazione) Direzione Assistenziale, AUSL-IRCCS di Reggio Emilia, Italia
Background and aims
Lymphedema is a chronic, progressive, and disabling condition caused by impaired lymphatic transport, often resulting in substantial functional limitations and reduced autonomy.
As with many chronic conditions, its management entails considerable healthcare expenditures. Current literature advocates for organizational models that enhance patient participation in the continuum of care.
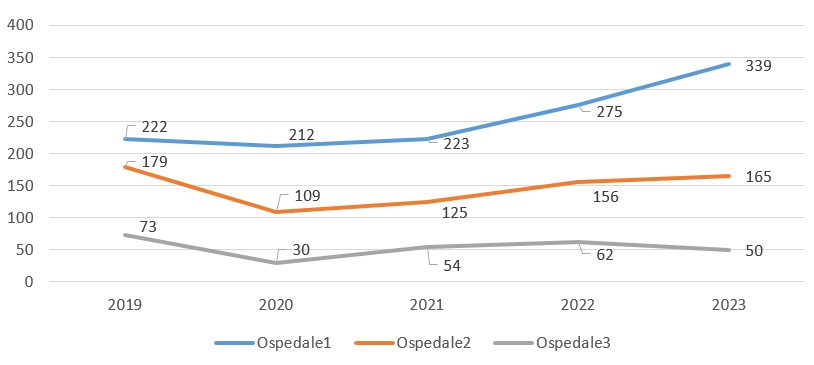
Institutional monitoring data indicate that, following completion of the physiotherapy cycle, patients frequently initiate informal contact with physiotherapists—typically in response to symptom recurrence or to request advice on newly arising concerns.
Methods
Within the existing territorial lymphedema rehabilitation network, a structured rehabilitative counseling service has been designed. The service is accessible via a secure digital platform, with the objective of formalizing, tracking, and expanding access to such informal consultations.
This direct-access model aims to offer timely and appropriate responses to low-complexity rehabilitation needs. Each patient may access the service for up to two consultations—either in person or via telemedicine—allowing the physiotherapist to assess the case and propose suitable interventions. In cases requiring more comprehensive care, the physiotherapist may directly initiate referral for physiatric evaluation.
Results
The launch of the rehabilitative counseling service is scheduled for Autumn 2025, with an initial pilot phase involving two healthcare districts.
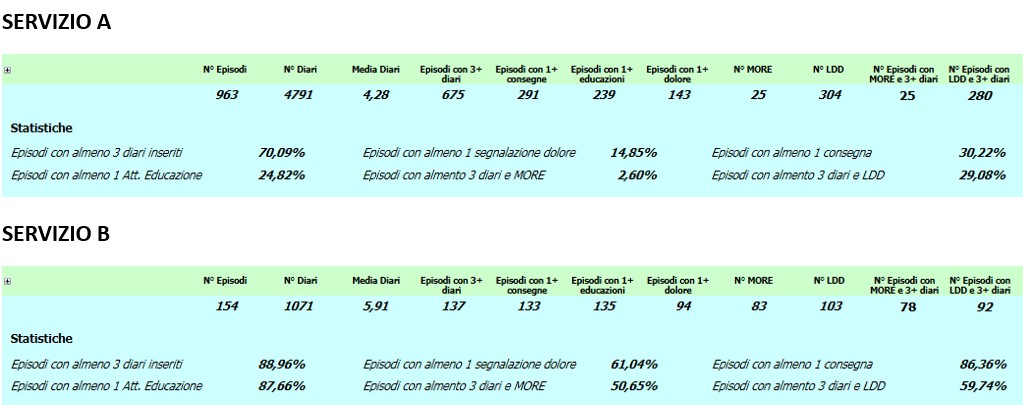
Service requests will be managed through a secure online form, serving as the user interface for access. The structure of this form will be informed by observational data collected from patients who currently engage the service informally.
Preliminary data suggest that the most frequently reported needs include: counseling on compression garments and bandaging techniques, verification of appropriate use of assistive devices, symptom self-management support, and lifestyle education.
During the first year of implementation, the service is expected to handle approximately 100 requests, with over 50% of cases likely to be managed autonomously by physiotherapists, without requiring referral for physiatric consultation.
In the long term, this model aims to reduce both the number of physiatric referrals and physiotherapy sessions for this patient population by approximately 10%.
Additional indicators will be monitored to evaluate the model’s effectiveness, including: case typology, nature of the interventions provided, response times, and user satisfaction, leveraging data generated through the digital request platform.
Conclusion
The activation of a lymphedema counselling service represents an innovative model of care, based on therapeutic education, self-management and proximity of the intervention, accordig with DM 77/2022. The project enhances the physiotherapist as a territorial reference point within the lymphological network, helping to reduce inappropriate access to physiatric visits and repeated treatments.
REFERENCES
- Gyawali B, Bowman M, Sharpe I, Jalink M, Srivastava S, Wijeratne DT. (2023) A systematic review of eHealth technologies for breast cancer supportive care. Cancer Treatment 2023; 114: 102519.
- Henkin JS, Botton CE, Simon MS, et al. Telehealth multicomponent exercise and health education in breast cancer patients undergoing primary treatment: rationale and methodological protocol for a randomized clinical trial (ABRACE: Telehealth). Trials. 2023; 24: 42.
- Hernandez Silva E, Lawler S, Langbecker D. The effectiveness of mHealth for self-management in improving pain, psychological distress, fatigue, and sleep in cancer survivors: a systematic review. Journal of Cancer Survivorship. 2019; 13: 97-107.