Passaggio dalla diagnosi basata sugli item a quella sul punteggio totale nella Coma Recovery Scale–Revised: uno studio di accuratezza diagnostica
Autori
Caselli Serena (Unità Operativa Complessa di Medicina Riabilitativa, Azienda Ospedaliero-Universitaria di Modena, Modena, Italy)
Pellicciari Leonardo (IRCCS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italy)
Leonardi Matilde (SC Neurologia, Salute Pubblica, Disabilità, Fondazione IRCCS Istituto Neurologico Carlo Besta, Milan, Italy)
Magnani Francesca Giulia (SC Neurologia, Salute Pubblica, Disabilità, Fondazione IRCCS Istituto Neurologico Carlo Besta, Milan, Italy)
Cacciatore Martina (SC Neurologia, Salute Pubblica, Disabilità, Fondazione IRCCS Istituto Neurologico Carlo Besta, Milan, Italy)
Barbadoro Filippo (SC Neurologia, Salute Pubblica, Disabilità, Fondazione IRCCS Istituto Neurologico Carlo Besta, Milan, Italy)
Ippoliti Camilla (SC Neurologia, Salute Pubblica, Disabilità, Fondazione IRCCS Istituto Neurologico Carlo Besta, Milan, Italy)
Kreiner Svend (Section of Biostatistics, Department of Public Health, University of Copenhagen, Copenhagen, Denmark)
La Porta Fabio (IRCCS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italy)
Background and aims
The Coma Recovery Scale-Revised (CRS-R) is the gold standard for diagnosing patients with Disorder of Consciousness (DOC). Five items out of six provide scores linked to a diagnosis of Unresponsive Wakefulness Syndrome (UWS), Minimally Conscious State (MCS), or emergence from MCS (eMCS). However, no diagnostic criteria are linked to the total score.
Therefore, this study proposes to define and compare the diagnostic accuracy of total score cutoffs based on item-level diagnostic criteria proposed recently[1] as a reference standard, and to improve the diagnostic accuracy of these total score cutoffs using a modified version of the original rule (i.e., the diagnostic category coincides with the highest category defined at least by one item)[2] currently in use.
Methods
Patients with DOC as a consequence of a severe acquired brain injury and admitted to post-acute and follow-up neuro-rehabilitation services were included. Diagnostic accuracy (DA) of the total score cutoffs based on each of the item-level diagnostic criteria set proposed recently[1-4], and the agreement indexes between item-level and total score-level diagnosis were computed. Finally, the comparison of the diagnostic accuracy of the total score cutoffs according to Giacino’s original rule[2] and the “modified rule” (i.e., the diagnostic category coincides with the highest category defined at least by two/three/four items) with Caselli’s criteria[1] was performed.
Results
380 patients with DOC (mean±SD: 52.1±16.8 years, 65% male) were included for a total of 727 CRS-R assessments.
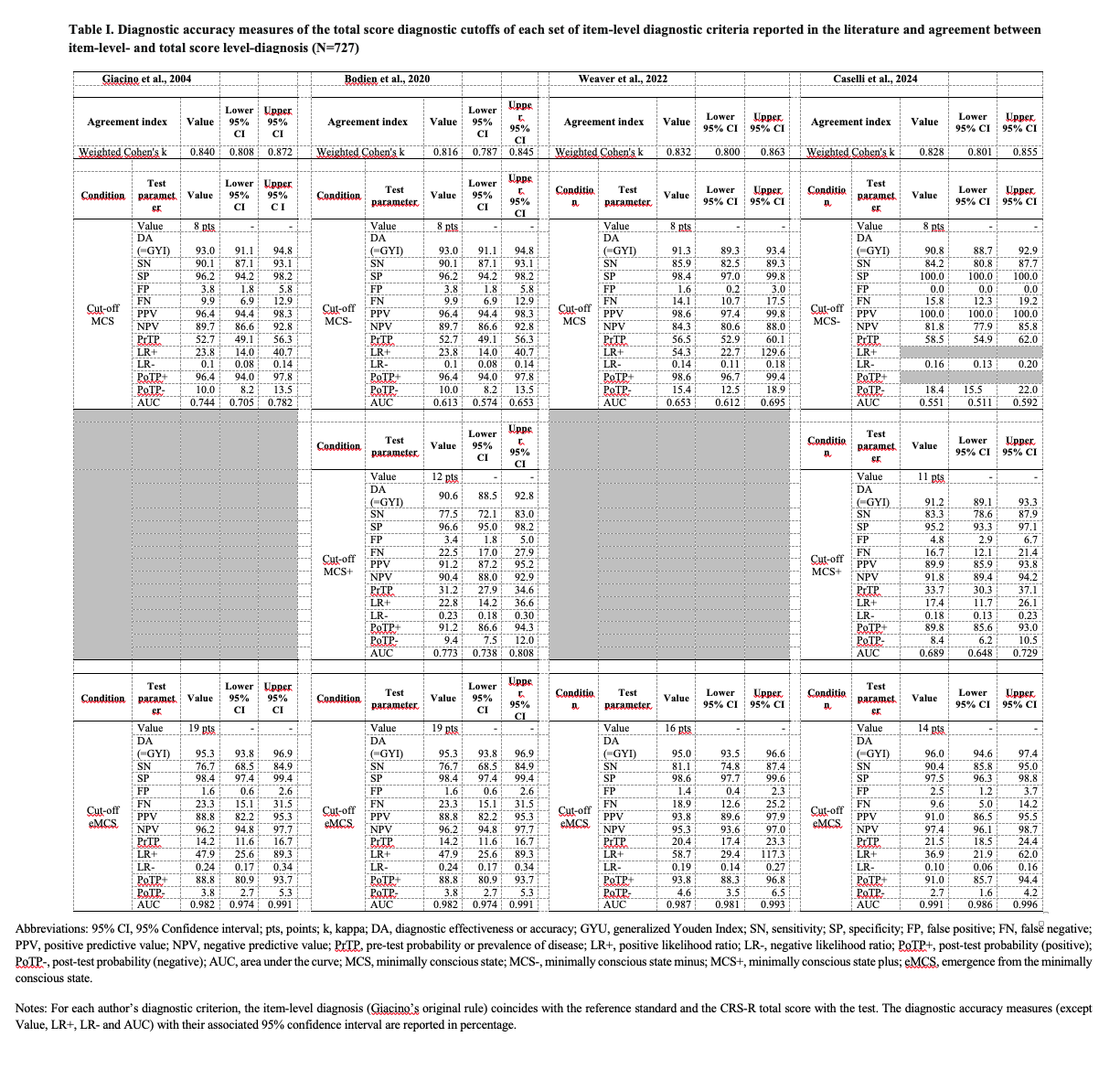
The comparison of total score cutoffs for each diagnostic criterion showed that for MCSplus and eMCS, the DA value is 90-95% (Table I), with high false negatives (FN) for most criteria sets (MCSplus: Bodien 12pt 22.5%; Caselli 11pt 16.7%; eMCS: Giacino and Bodien 19pt 23%; Weaver 16pt 19%). For MCSminus, the four cutoffs (8pt) had high specificity, essential for identifying patients with early signs of consciousness. Weighted Cohen’s k between the item and total score diagnoses was 0.82 for all four criteria sets.
Applying the “modified rule” with Caselli’s criteria resulted in the highest DA values for both MCSplus (14pt 97%) and eMCS (19pt 99%), with a lower FN rate (<11%) (Tables II and III).
Conclusion
Being the diagnosis based on individual items, the initial total score cutoffs partly addressed the low reliability of item-level cutoffs. The introduction of the “modified rule,” which requires at least two items per diagnostic category for diagnosis, allowed for advancing from item-level to a reliable total score-based diagnosis with less measurement error.
REFERENCES
- Caselli S, Leonardi M, Magnani FG, Cacciatore M, Barbadoro F, Ippoliti C, Kreiner S, Pellicciari L, La Porta F. Comparing the Different Sets of Item-Level Diagnostic Criteria of the Coma Recovery Scale-Revised (CRS-R): A Measurement-Based Approach Driven by Rasch Analysis. Arch Phys Med Rehabil. 2024 Dec 18:S0003-9993(24)01406-0. doi: 10.1016/j.apmr.2024.12.009.
- Giacino JT, Kalmar K, Whyte J. The JFK Coma Recovery Scale-Revised: measurement characteristics and diagnostic utility. Arch Phys Med Rehabil. 2004 Dec;85(12):2020-9. doi: 10.1016/j.apmr.2004.02.033.
- Bodien YG, Chatelle C, Taubert A, Uchani S, Giacino J T, Ehrlich-Jones L. Updated measurement characteristics and clinical utility of the Coma Recovery Scale-Revised among individuals with acquired brain injury. Arch Phys Med Rehabil. 2021;102(1):169-171. doi: 10.1016/j.apmr.2020.09.369.
- Weaver JA, Cogan AM, O’Brien KA, Hansen P, Giacino JT, Whyte J, Bender Pape T, van der Wees P, Mallinson T. Determining the Hierarchy of Coma Recovery Scale-Revised Rating Scale Categories and Alignment with Aspen Consensus Criteria for Patients with Brain Injury: A Rasch Analysis. J Neurotrauma. 2022 Oct;39(19-20):1417-1428. doi: 10.1089/neu.2022.0095.