Benefici e rischi della Terapia Manipolativa Spinale nel trattamento del dolore cervicale aspecifico recente e persistente: una revisione sistematica con meta-analisi
Benefits and harms of Spinal Manipulative Therapy for treating recent and persistent nonspecific neck pain: a systematic review with meta-analysis
Autori
Silvia Minnucci [Department of Clinical Science and Translational Medicine, University of Rome Tor Vergata, Rome, Italy]
Tiziano Innocenti [Department of Health Sciences, Faculty of Science, Vrije Universiteit Amsterdam, Amsterdam Movement Sciences, The Netherlands]
Stefano Salvioli [Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genova, Campus of Savona, Italy],
Silvia Giagio [Department of Biomedical and Neuromotor Sciences (DIBINEM), Alma Mater Studiorum, University of Bologna, Bologna, Italy]
Marzia Stella Yousif [Department of Clinical Science and Translational Medicine, University of Rome Tor Vergata, Rome, Italy]
Daniel Feller [Provincial Agency for Health of the Autonomous Province of Trento, Trento, Italy]
Fabrizio Brindisino [Department of Medicine and Health Science “Vincenzo Tiberio”, University of Molise c/o Cardarelli Hospital, C/da Tappino 86100 Campobasso, Italy]
Agostino Faletra [Queen Elizabeth Hospital, Clinical Support & Screening Service, Gateshead, United Kingdom]
Alessandro Chiarotto [Department of Health Sciences, Faculty of Science, Vrije Universiteit Amsterdam, Amsterdam Movement Sciences, The Netherlands]
Firas Mourad [Department of Health, LUNEX University, 4671 Differdange, Luxembourg].
Introduction
Neck pain (NP) is one of the most common and disabling musculoskeletal conditions. Different clinical practice guidelines (CPGs) provide contradictory recommendations for how to manage NP, likely because of the low-quality evidence. Cervical spinal manipulative therapy (SMT), considered to represent both non-thrust mobilization and thrust manipulation, is a common intervention for NP within a multimodal care pathway. Overall, the effectiveness of cervical SMT for reducing pain and disability varies between studies and their results depend on symptoms staging, outcomes, comparators, and whether combined with other interventions. There is plenty of debate regarding manual therapy; some call for clinicians to abandon SMT. Therefore, clinicians need trustworthy information about the safety and effectiveness of the intervention.
The objective of this systematic review with meta-analysis of randomized controlled trials is to estimate the benefits and harms of cervical SMT for treating NP.
Methods
This systematic review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) on 30 April 2021 (registration number CRD42021245671).
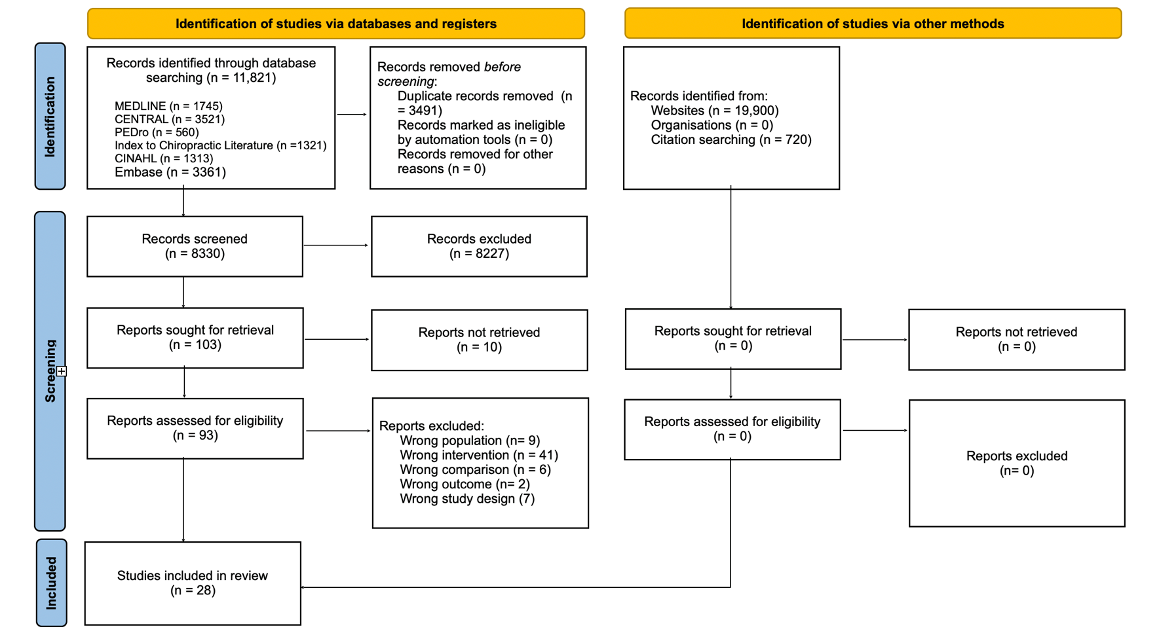
We searched the MEDLINE, Cochrane CENTRAL, EMBASE, CINAHL, PEDro, Chiropractic Literature Index bibliographic databases, and grey literature sources, up to June 6, 2022.
Randomized controlled trials (RCTs) evaluating SMT compared to guideline-recommended and non-recommended interventions, sham SMT, and no intervention for adults with neck pain were eligible for our systematic review.
Pre-specified outcomes included pain, range of motion, disability, health-related quality of life.
Random-effects meta-analysis for clinically homogeneous RCTs at short-term and long-term outcomes.
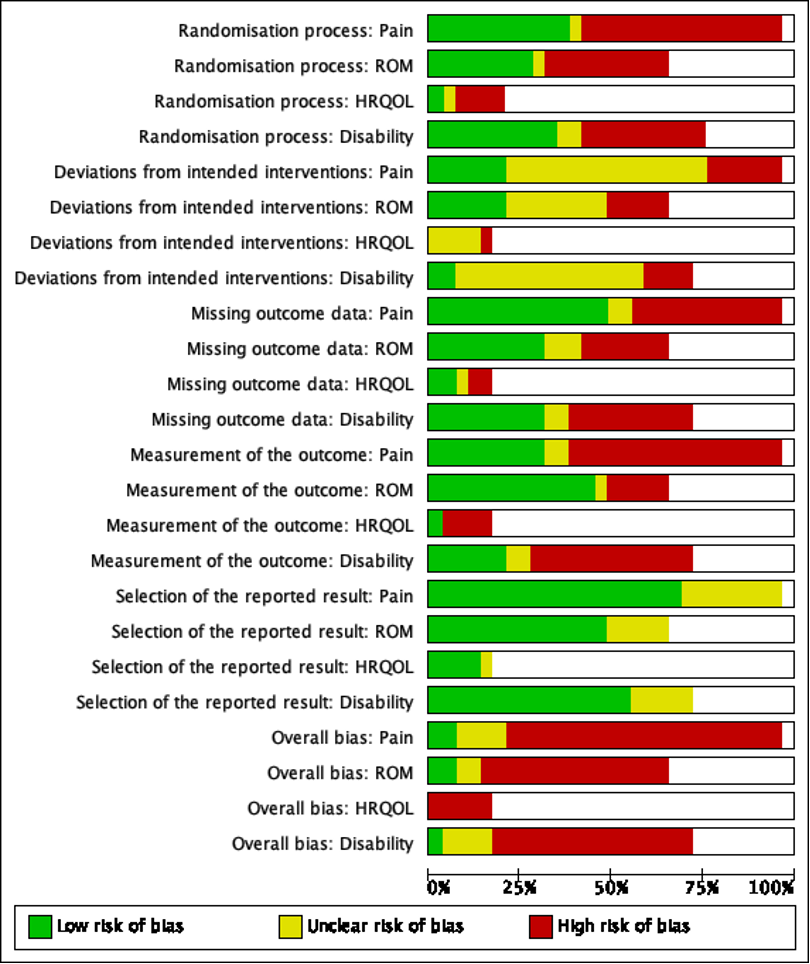
Risk of bias was assessed using the Cochrane Risk-of-Bias 2.0 Tool.
We used the Grading of Recommendations Assessment Development and Evaluation approach to judge the certainty of evidence.
Results
We included 28 RCTs with a total number of 2139 patients.
Two trials were at an overall “low risk” of bias, four had “some concerns.” The remaining 22 trials were at “high risk” of bias for all the investigated outcomes.
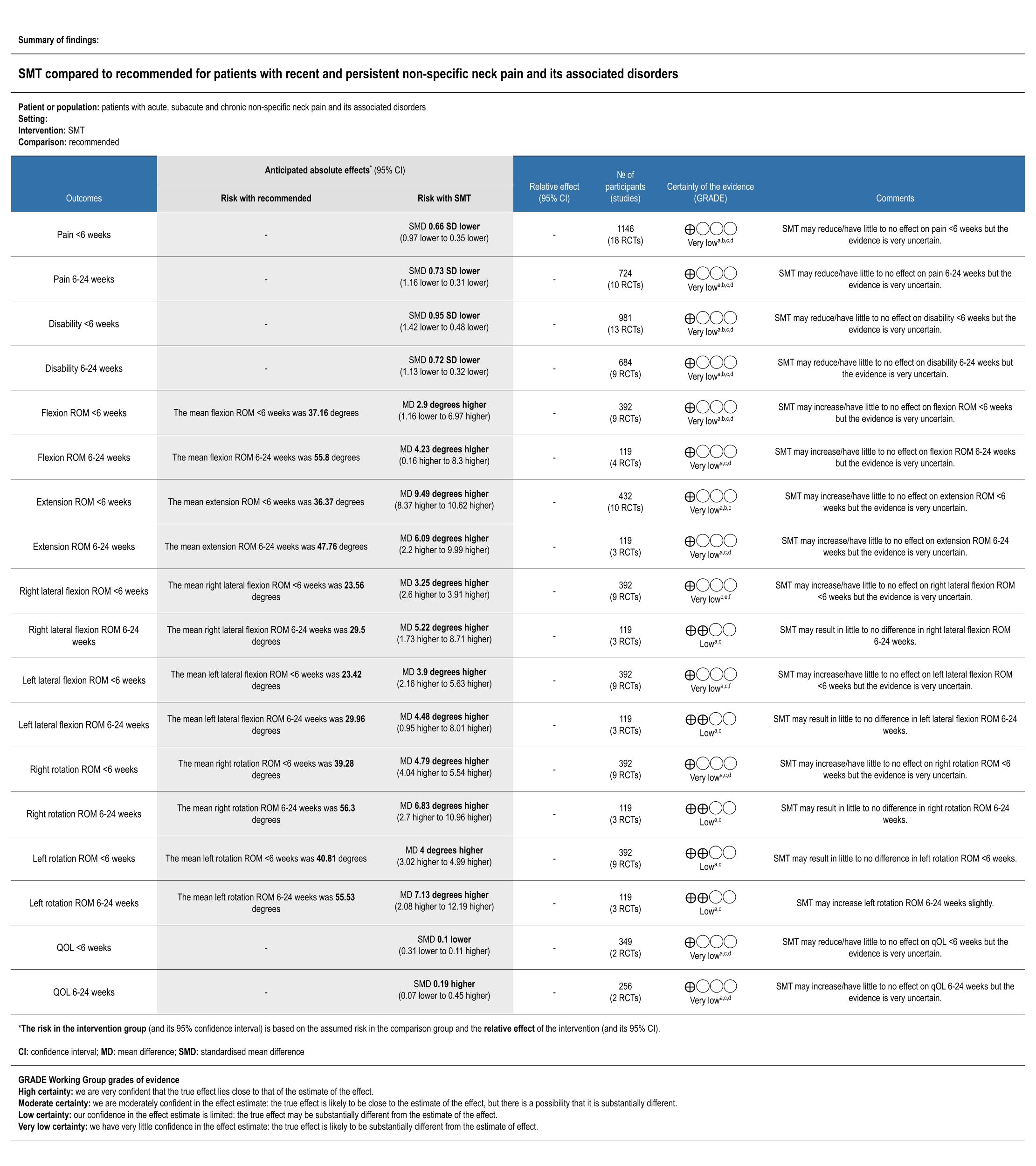
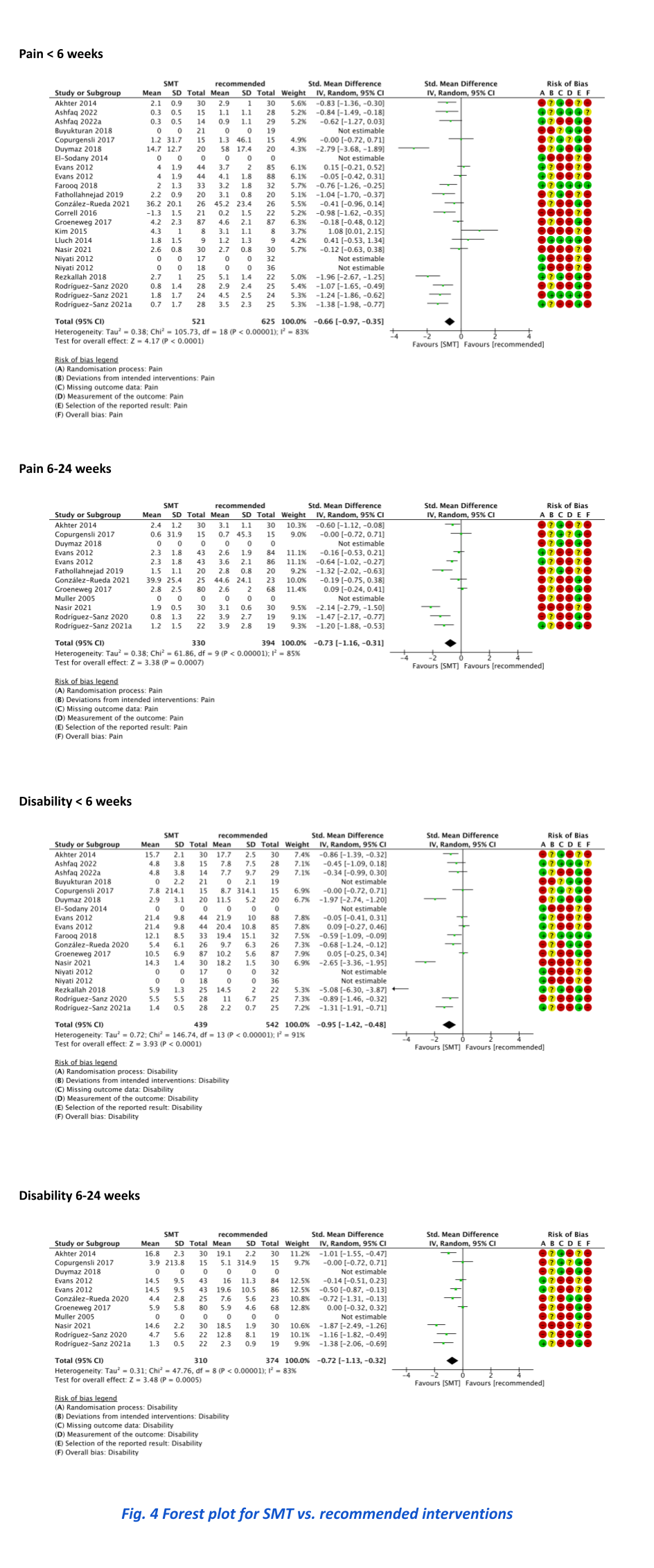
There was very low to low certainty evidence that SMT was more effective than recommended interventions for improving pain at short-term (standardized mean difference [SMD] 0.66; confidence interval [CI] 0.35 to 0.97) and long-term (SMD 0.73; CI 0.31 to 1.16), and for reducing disability at short-term (SMD 0.95; CI 0.48 to 1.42) and long-term (SMD 0.65; CI 0.23 to 1.06). Transient side effects only were found (e.g., muscle soreness).
Discussion and Conclusion
Our results should be interpreted cautiously as the certainty of evidence varied from very low to low. We found that cervical SMT results in statistically significant and clinically relevant short- and long-term effects compared to recommended interventions for pain and disability. Non-statistically significant effects were found for pain and disability compared to non-recommended interventions, and statistically significant short-term effects were found on disability compared to sham and no interventions. Cervical SMT may provide ROM improvement, especially for extension, rotation, and lateral flexion movements. No differences were found between mobilization and thrust manipulation, except rotational ROM for thrust manipulation. Only a few trials reported minor AEs with the lowest proportion of side effects compared to exercise.
In conclusion there was very low certainty evidence supporting cervical SMT as an intervention to reduce pain and improve disability in people with neck pain.
REFERENCES
Ferrari R, Russell AS. Regional musculoskeletal conditions: neck pain. Best Pract Res Clin Rheumatol. 2003;17:57-70.
Gross A, Miller J, D’Sylva J, et al. Manipulation or mobilisation for neck pain. Cochrane Database Syst Rev. 2010;CD004249.
Parikh P, Santaguida P, Macdermid J, Gross A, Eshtiaghi A. Comparison of CPG’s for the diagnosis, prognosis and management of non-specific neck pain: a systematic review. BMC Musculoskelet Disord. 2019;20:81
Rubinstein SM, de Zoete A, van Middelkoop M, Assendelft WJJ, de Boer MR, van Tulder MW. Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain: systematic review and meta-analysis of RCTs. BMJ. 2019;364:l689.
Sterne JAC, Savovic J, Page MJ, et al. RoB 2: a revised tool for assessing RoB in randomised trials. BMJ. 2019;366:l4898.
Schünemann H, Brożek J, Guyatt G, Oxman A, editors. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2021. The GRADE Working Group, 2013.