Recupero dello sbilanciamento durante il cammino
Recovery of gait perturbation
Autori
Maurizio Petrarca (Movement Analysis and Robotics Laboratory (MARlab), Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy)
Martina Favetta (Movement Analysis and Robotics Laboratory (MARlab), Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy)
Sacha Carniel (Movement Analysis and Robotics Laboratory (MARlab), Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy)
Simone Gazellini (Movement Analysis and Robotics Laboratory (MARlab), Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy)
Azzurra Speroni (Movement Analysis and Robotics Laboratory (MARlab), Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy)
Gessica della Bella (Movement Analysis and Robotics Laboratory (MARlab), Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy)
Lettori Donatella (Movement Analysis and Robotics Laboratory (MARlab), Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy)
Susanna Summa (Movement Analysis and Robotics Laboratory (MARlab), Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy)
Alain Berthoz (Laboratoire de Physiologie de la Perception et de l’Action, Collège de France, 11, rue Marcelin Berthelot, 75005 Paris, France)
Introduction
Walking is characterised by the ability to adapt the function to dynamical events derived from internal and external body perturbations. Gait perturbations could arise from irregular terrain, leading to expected or unexpected disturbances which are compensated by Anticipatory, Predictive and Reactive strategies [1]. Compensation abilities are compromised in pathological conditions [2], meanwhile, they are still developing in children. The purpose was to detect gait strategies and the key joints involved in the counter-reacting perturbation.
Methods
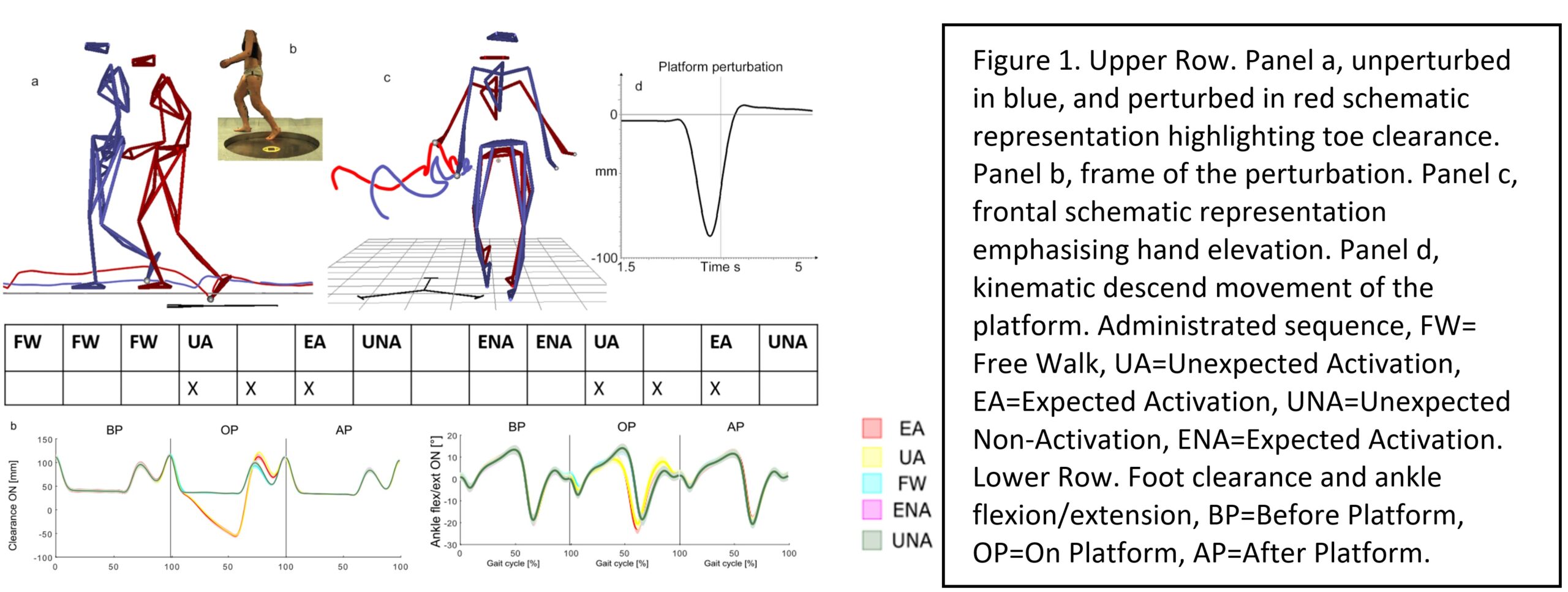
To address this question, we developed an ad-hoc robotized platform (Mufy, IT) for inducing perturbations during walking [3]. We recruited ten healthy young adults (3 males and 7 females, with a mean age of 31 ± 7 years). Participants walked along a path where the upper plate of a Stewart Platform was camouflaged. A control in force moved the platform vertically downward when participants stepped on it. The fall down of the platform was normalized based on the leg length and mass of the participants personalizing the stiffness of the simulated spring. The platform descended 10% of the leg length. The sequence repetition to induce expected or unexpected conditions was defined (See Figure 1, Upper Row). Each sequence was repeated with both legs. We conducted a full body 3D gait analysis of three strides before, on, and after the platform using an optoelectronic system with 12 cameras (Vicon, UK) to gather kinematics data.
Results
Statistical analysis was performed using one-dimensional Statistical Parametric Mapping to compare perturbed conditions (both expected or unexpected) to normal walking. The main findings revealed alterations in spatiotemporal parameters (p<0.0001), increased clearance (p<0.02 expected perturbation, p<0.01 unexpected perturbation, p<0.009 for unexpected non-activation), and increased dorsiflexion of the ankle (p<0.001) (see Figure 1, Lower Row), with minor effects on knee and hip flexion, hands elevation and anteversion of pelvis and trunk.
Discussion and Conclusion
In summary, our observations indicated an overlap between Anticipatory and Predictive strategies. Nevertheless, we find evidence of Anticipatory strategies looking at the increased foot clearance during the unexpected absence of perturbation and signs of Predictive strategies looking at hand elevation during the presence of perturbation. The perturbations were mainly absorbed at the ankle level raising the importance of focusing on this joint to assess the residual ability for gait compensation.
REFERENCES
[1] Patla, A. EEE Eng in Med and Biology Magazine, 22(2), 48-52 (2003).
[2] Pacilli, A. et al. Gait Posture 42, S4–S5 (2015).
[3] Summa, S. et.al. Sensors, 19, 3402 (2019).