Responsività alla riabilitazione della stabilità dinamica locale del tronco in soggetti con atassia cerebellare degenerativa primaria.
Responsiveness to rehabilitation of local dynamic stability of the trunk in subjects with primary degenerative cerebellar ataxia.
Autori
Castiglia Stefano Filippo [Department of Medico-Surgical Sciences and Biotechnologies, “Sapienza” University of Rome-Polo Pontino, Latina, Italy; Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy]]
Trabassi Dante [Department of Medico-Surgical Sciences and Biotechnologies, “Sapienza” University of Rome-Polo Pontino, Latina, Italy]
Conte Carmela [Department of Medico-Surgical Sciences and Biotechnologies, “Sapienza” University of Rome-Polo Pontino, Latina, Italy]
Varrecchia Tiwana [Department of Occupational and Environmental Medicine, Epidemiology and Hygiene, INAIL, Monteporzio Catone, Italy]
Chini Giorgia [Department of Occupational and Environmental Medicine, Epidemiology and Hygiene, INAIL, Monteporzio Catone, Italy]
Ranavolo Alberto [Department of Occupational and Environmental Medicine, Epidemiology and Hygiene, INAIL, Monteporzio Catone, Italy]
Casali Carlo [Department of Medico-Surgical Sciences and Biotechnologies, “Sapienza” University of Rome-Polo Pontino, Latina, Italy]
Serrao Mariano [Department of Medico-Surgical Sciences and Biotechnologies, “Sapienza” University of Rome-Polo Pontino, Latina, Italy; Movement Analysis Lab, Policlinico Italia, Roma]
Introduction
Ataxic gait is characterized by incoordination between the upper and lower bodies, which results in increased upper body oscillations with a lack of local trunk stability, transforming the trunk into a generator of perturbations during walking [1]. Recently three trunk acceleration – derived gait indexes, namely the harmonic ratios (HRs), short-time longest Lyapunov’s exponent (sLLE), and step-to-step coefficient of variation (CV), showed the best ability to characterize the trunk behavior during gait of swCA[2,3]. This study aimed to assess the responsiveness to the rehabilitation of HR, sLLE, CV in a sample of subjects with primary degenerative cerebellar ataxia (swCA), and investigate the correlations between their improvements (∆), clinical characteristics, and spatio-temporal and kinematic gait features.
Methods
The trunk acceleration patterns in the antero-posterior (AP), medio-lateral (ML), and vertical (V) directions during gait of 21 swCA were recorded using a magneto-inertial measurement unit placed at the lower back before (T0) and after (T1) a period of inpatient rehabilitation. For comparison, a sample of 21 age- and gait speed-matched healthy subjects (HSmatched) was also included. Cohen’s d with Hedge’s correction was used to calculate internal responsiveness. To identify significant differences between swCA and HS at T0 and T1, the unpaired t-test or Mann–Whitney test was used. The external responsiveness was assessed using an anchor-based method using the smallest detectable change of the SARA scale (3.5 points) criterion for clinical improvement[4].
Results
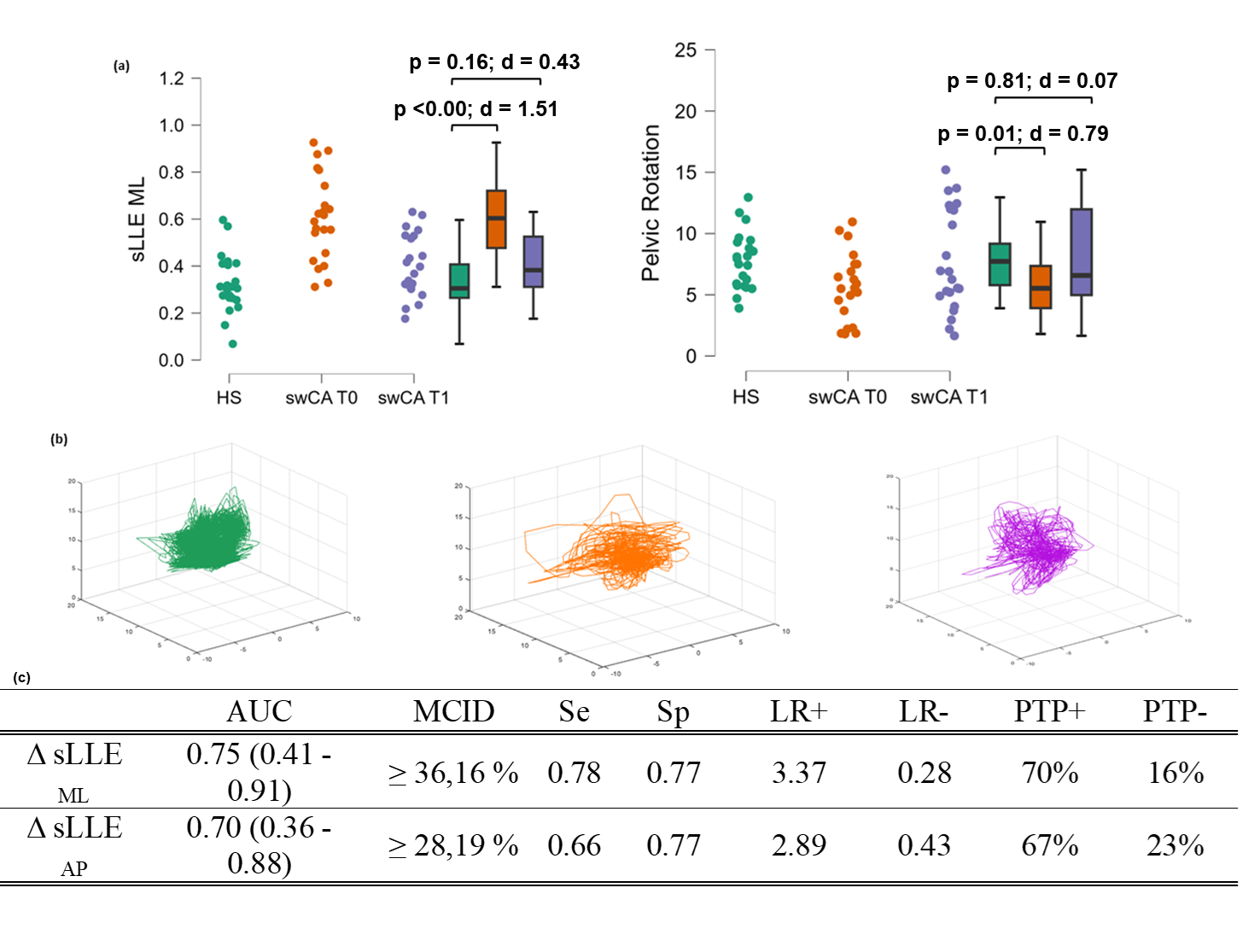
At T1, sLLE in the AP (sLLEAP) and ML (sLLEML) directions significantly improved with moderate to large effect sizes (sLLEAP: p = 0.03; d= 0.75; sLLEML: p=0.00; d = 0.86), as well as SARA scores (p = 0.00; d = 0.73), stride length (p = 0.04; d = 0.46), and pelvic rotation (p = 0.03; d = 0.49). sLLEML and pelvic rotation also approached the HSmatched values at T1 (Fig. 1, a), suggesting a normalization of the parameter. HRs and CV did not significantly modify after rehabilitation. ∆sLLEML correlated with ∆ of the gait subscore of the SARA scale (∆SARAGAIT) (ρ = 0.41; p = 0.03) and ∆stride length (ρ = 0.51; p = 0.01). ∆sLLEAP correlated with ∆pelvic rotation (ρ = 0.41; p = 0.03) and ∆SARAGAIT (ρ = 0.43; p = 0.03). The minimal clinically important differences (MCID) for sLLEML and sLLEAP were ≥ 36.16% and ≥ 28.19%, respectively, as the minimal score reflecting a clinical improvement in SARA scores (Fig. 1, c).
Discussion and Conclusion
sLLE in the ML and AP directions revealed good internal and external responsiveness, and moderately correlated with the improvements in SARAGAIT subscore, stride length, and pelvic rotation [5]. The findings of this study suggest that trunk stability can be effectively quantified using sLLE and improve after rehabilitation. Because of the usability and affordability of magneto-inertial measurement units, sLLE can be considered a useful additional outcome measure for assessing the effectiveness of intensive rehabilitation treatments, particularly when focusing on improvements in trunk stability during gait. Further studies including larger populations are needed to confirm these results and investigate long-term responsiveness.
REFERENCES
[1]Manto M, Serrao M, Filippo Castiglia S, Timmann D, et al. Neurophysiology of cerebellar ataxias and gait disorders. Clin Neurophysiol Pract. 2023 Jul 20;8:143-160.
[2]Castiglia SF, Trabassi D, Tatarelli A, et al. Identification of Gait Unbalance and Fallers Among Subjects with Cerebellar Ataxia by a Set of Trunk Acceleration-Derived Indices of Gait. Cerebellum. 2023 Feb;22(1):46-58.
[3]Caliandro P, Conte C, Iacovelli C, et al. Exploring Risk of Falls and Dynamic Unbalance in Cerebellar Ataxia by Inertial Sensor Assessment. Sensors (Basel). 2019 Dec 17;19(24):5571
[4]Schmitz-Hübsch T, Fimmers R, Rakowicz M, et al.Responsiveness of different rating instruments in spinocerebellar ataxia patients. Neurology. 2010 Feb 23;74(8):678-84
[5]Castiglia SF, Trabassi D, Conte C, et al. Local Dynamic Stability of Trunk During Gait is Responsive to Rehabilitation in Subjects with Primary Degenerative Cerebellar Ataxia. Cerebellum. 2024 Jan 27. doi: 10.1007/s12311-024-01663-4. Epub ahead of print.