CAUSAL DISPOSITIONALIST PSYCHOLOGICALLY-INFORMED PRACTICE COMBINED WITH MANUAL THERAPY IN A PATIENT WITH PERSISTENT NONSPECIFIC NECK PAIN (NS-NP): A CASE REPORT
Autori
Celso Andrea [Azienda sanitaria Friuli Occidentale, Pordenone, Italy]
Introduction to clinical case
Neck pain is one of the most common musculoskeletal disorders and is a major problem in modern society.
It can be considered a multifactorial disease with a point prevalence of between 10% and 40% of population that will experience symptoms in any one year.
In the following case report are shown the results of a combined physiotherapy treatment, merging manual therapy and functional rehabilitation with a psychologically-informed practice framework guided by a causal dispositionalist lens, including Motivational Interviewing (MI), Mindfulness-based Therapy with Acceptance and Commitment Therapy (ACT).
Methods
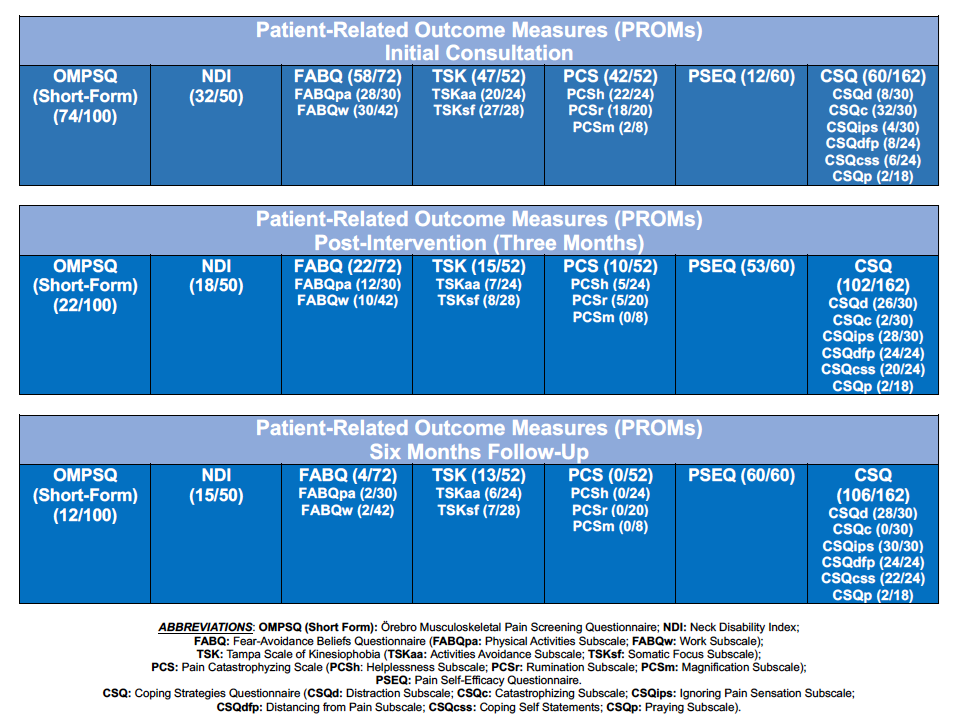
n 1 female, 58-years-old industry secretary, with a one year history of persistent nonspecific neck pain was treated in three months period and evaluated with initial, post-intervention screening and one-year follow-up, with administration of Patient-Related Outcome Measures such as Örebro Musculoskeletal Pain Screening Questionnaire (OMPSQ) and consequent further functional, and psychosocial assessment with Neck Disability Index (NDI), Fear-Avoidance Beliefs Questionnaire (FABQ), Tampa Scale of Kinesiophobia (TSK), Pain Catastrophizing Scale (PCS), Coping Strategies Questionnaire (CSQ) and Pain Self Efficacy Questionnaire (PSEQ), as measures to evaluate patient’s clinical profile, engagement in treatment and self-management strategies learning.
The therapeutic encounters were characterized by the implementation of specific manual techniques addressed to the cervical and thoracic spine merged with therapeutic exercise to reduce pain hypersensitivity and restore functional movements.
Results
A dispositionalist patient-centred and psychologically informed practice clinical reasoning framework guided the therapeutical journey, where specific manual techniques Motivational Interviewing (MI), Mindfulness and ACT principles enabled to improve psychological flexibility and enhance personal engagement and self-management activation at the end of therapeutic program and at one-year follow-up, at outcomes re-evaluation comparing to baseline.
Discussion and clinical relevance
In persistent pain states the therapeutic pathway should be shaped towards a multidimensional framework whose the main objective is to reach meaning(s) of pain experience, where the uniqueness of single clinical presentation can be effectively met and managed. Further, be acquainted in Mindfulness and ACT’s core principles, directly reduces avoidance and promote openness, bringing the possibility to build present-focused awareness, and coordinate greater engagement in goal-oriented and values-based activities, representing a good viaticum that prompt patient’s recovery and thrive.
REFERENCES
- Sterling, Michele. Neck pain: much more than a psychosocial condition. JOSPT. 2009;39(5):309-311.
- Bernal-Utrera C, Gonzalez-Gerez JJ, Anarte-Lazo E, Rodriguez-Blanco C. Manual therapy versus therapeutic exercise in non-specific chronic neck pain: a randomized controlled trial.Trials. 2020;21, 1-10.
- Worsfold C. Functional rehabilitation of the neck. Phys Ther Rev. (2020);25(2):61-72.
- Anjum RL, Copeland S, Rocca, E. Rethinking causality, complexity and evidence for the unique patient: A CauseHealth resource for healthcare professionals and the clinical encounter. Springer 2020.
- Main CJ, Simon CB, Beneciuk JM, Greco CM, George SZ, Ballengee LA. The psychologically informed practice consultation roadmap: a clinical implementation strategy.Phys Ther. 2023;103(7), pzad048.