Alterazioni nella gait initiation dopo frattura di arto inferiore: la fisioterapia può prevenire l’apprendimento al non uso?
Changes in gait initiation after lower limb immobilization: can physiotherapy prevent “learning non-use”?
Autori
Sgubin Giulia (Department of Life Science, University of Trieste, Trieste, Italy; ASUGI, Trieste, Italy; Department of Medicine, Surgery and Health Sciences, University of Trieste, Trieste, Italy)
Trobec Belinda (Department of Medicine, Surgery and Health Sciences, University of Trieste, Trieste, Italy; ASUGI, Trieste, Italy)
Canton Gianluca (Department of Medicine, Surgery and Health Sciences, University of Trieste, Trieste, Italy; ASUGI, Trieste, Italy)
Zelesnich Francesca (Department of Medicine, Surgery and Health Sciences, University of Trieste, Trieste, Italy; ASUGI, Trieste, Italy)
Sabot Raffaele (Department of Medicine, Surgery and Health Sciences, University of Trieste, Trieste, Italy; ASUFC, Udine, Italy)
Deodato Manuela (Department of Medicine, Surgery and Health Sciences, University of Trieste, Trieste, Italy; ASUGI, Trieste, Italy)
Murena Luigi (Department of Medicine, Surgery and Health Sciences, University of Trieste, Trieste, Italy; ASUGI, Trieste, Italy)
Introduction
The effects of inactivity and lack of load following a lower limb fracture on motor behavior are well known [1]. Walking and transitional movements such as gait initiation are bipedal activities in which load is progressively transferred between the two lower limbs within a variable base of support depending on the action [2].
The lack of load after a fracture or lower limb surgery results in impaired load management, leading to reduced smoothness in body progression during walking.
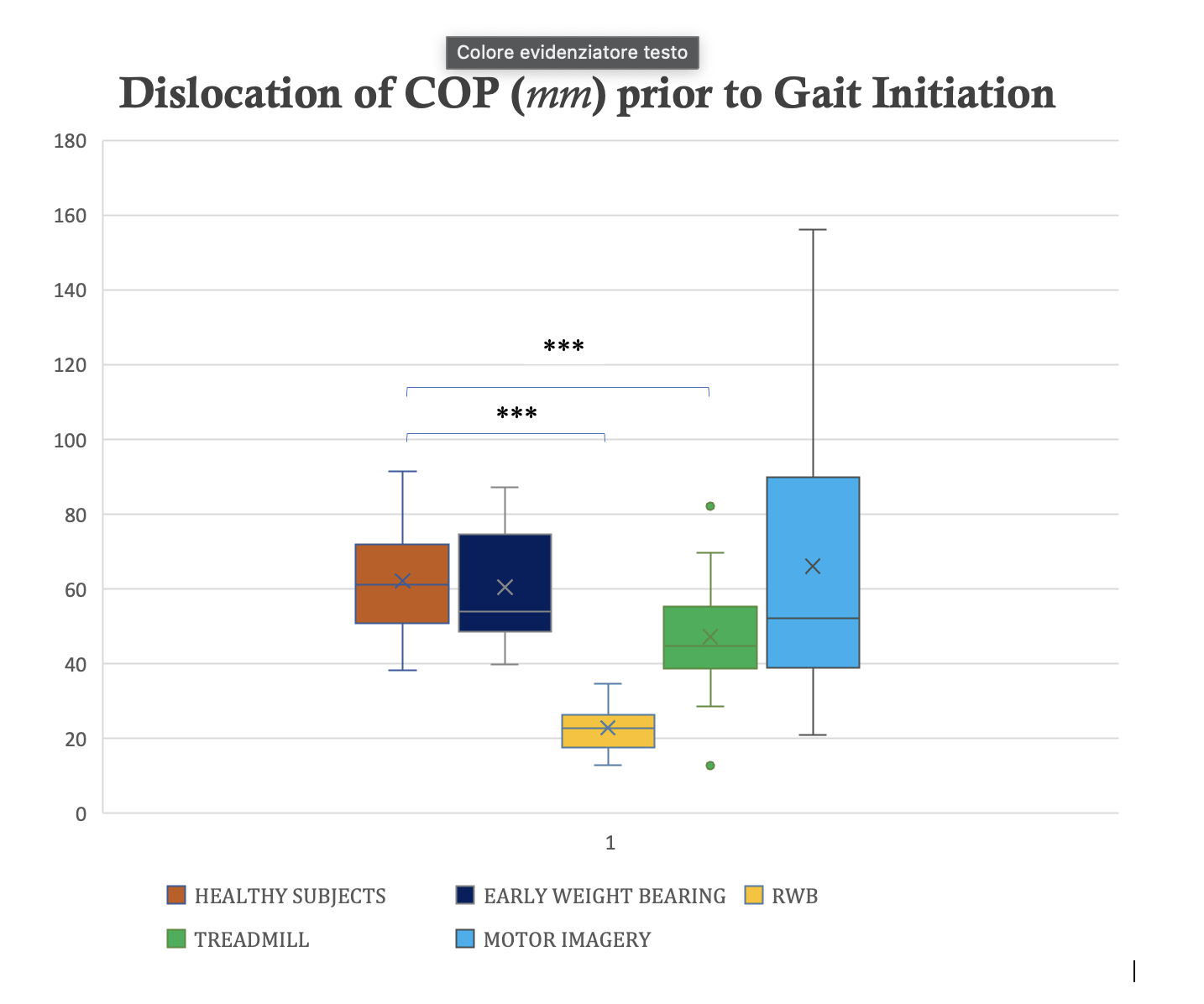
This study analyzed the center of pressure (COP) lateral displacement prior to self-generated gait initiation.
Methods
Four groups of individuals with lower limb fractures were compared to a group of healthy.
RWB group comprised patients who, according to healthcare system, did not access physiotherapy until weight-bearing was permitted.
EWB group included patients who were operated on and immediately ready for weight-bearing on the operated limb.
MOTOR IMAGERY group consisted of non-weight-bearing patients who were offered motor imagery exercises in combination with early rehabilitation.
TREADMILL group included non-weight-bearing patients who received early rehabilitation and antigravity treadmill simulating walking without gravity.
Subjects underwent clinical and functional evalutation and gait analysis at 3 months post-fracture; all subjects fully bear weight on both lower limbs.
Data related to the COP lateral displacement preceding the heel-off were recorded in motion analysis laboratory using an optoelectronic system. Subjects were instructed to initiate walking with the limb that had the fracture.
Results
The analysis of the collected data identified a significant reduction in COP displacement during medio-lateral phase of anticipatory postural adjustments (APAs) after the period of inactivity in RWB and TREADMILL groups compared to the group of healthy subjects and the group of patients with early weight-bearing (P<.00001).
EWB and MOTOR IMAGERY groups demonstrated a behavior similar to that of healthy subjects as early as 3 months post-operation (P=.92828 and P=.71138).
Discussion and Conclusion
The study highlighted the impaired load management in the groups of patients with lower limb fracture after cast immobilization during the task of gait initiation. Considering that the anticipatory postural adjustment (APA) occurred on the contralateral lower limb, these data support the line of studies [3] suggesting that motor behavior alterations, even in the presence of a fracture or “peripheral damage”, affect central movement control mechanisms.
Furthermore, the study has allowed for the identification and quantification of movement strategies that are not otherwise measurable but are only observable in a clinical setting and persist in these patients despite the progressive recovery of weight-bearing.
REFERENCES
[1] Moisello C, et al. J Mot Behav. 2008;(40):165–176.
[2] Winter DA. Gait Posture. 1995;(3):193–214.
[3] Ebrahimabadi Z et al. Journal of Bodywork and Movement Therapies 2018;22(1):40–5.