Prevalenza del dolore neuropatico tra pazienti in accordo con il grading system aggiornato e nuovi cut-off dei questionari.
Prevalence of neuropathic pain among patients according to the updated grading system and new questionnaires’ cut-offs.
Autori
Cavicchi Tommaso [Department of Clinical Sciences and Translation Medicine, University of Rome “Tor Vergata”, 00133 Rome, Italy]
Esposto Massimo [Department of Medicine and Health Science “Vincenzo Tiberio”, University of Molise, c/o Cardarelli Hospital, C/da Tappino, 86100 Campobasso, Italy]
Zanoli Gustavo [Orthopaedic Unit, Santa Maria Maddalena Hospital.Via Gorizia 2, 45030 Occhiobello (Ro), Italy]
Sindaco Gianfranco [Interdisciplinary Pain Unit,Santa Maria Maddalena Hospital.Via Gorizia 2, 45030 Occhiobello (Ro), Italy; Advanced Algology Research, Via Monttefeltro 66, Rimini, Italy]
Polli Andrea [Pain in Motion (PiM) international research group, Department of Physiotherapy, Human Physiology and Anatomy, Faculty of Rehabilitation Sciences & Physiotherapy, Vrije Universiteit Brussel, Brussels, Belgium; www.paininmotion.be; Department of Public Health and Primary Care, Centre for Environment & Health, KU Leuven, Leuven, Belgium; Flanders Research Foundation – FWO]
Introduction
Neuropathic pain (NP) is characterized by intense symptoms, a longer prognosis, and different management strategies when compared to other pain presentations. Early diagnosis of NP is crucial to improve clinical outcomes and follows the International Association for the Study of Pain (IASP) grading system, which classifies NP likelihood as “possible”, “probable”, and “definite”. Several tools have been developed and described in the literature to aid the process of diagnosing NP, such as the Leeds Assessment of Neuropathic Symptoms and Signs (LANSS), and painDETECT. However, it is still unclear to what extent these tools could help clinicians to assess patients presenting with features of NP. Therefore, this work aimed to determine the prevalence of NP pain among patients who present to a private clinic, assess the accuracy of LANSS and painDETECT compared to the updated IASP grading system, and explore correlations between questionnaires’ scores and clinical variables.
Methods
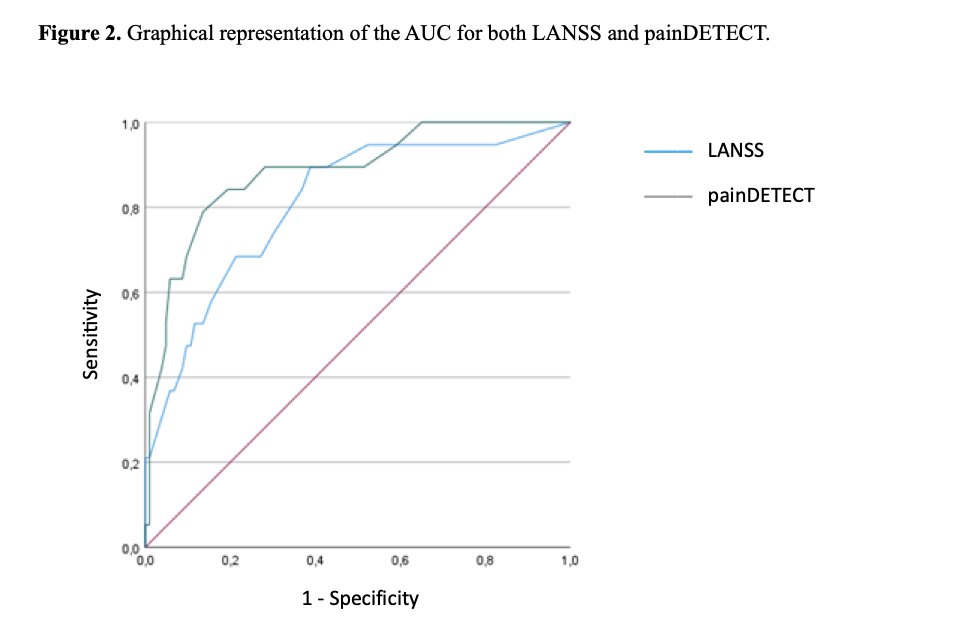
Consecutive patients presenting to two private clinics from July 2018 to December 2019 were assessed by a medical doctor according to the updated IASP grading system for NP. Two blinded physiotherapists collected demographic data, questionnaires’ scores (i.e., LANSS, painDETECT), and clinical variables (e.g., quality of life). The non-parametric Bonferroni-corrected Kruskal-Wallis test was run to check for intergroup differences. Received Operating Characteristics (ROC) and Areas Under the Curve (AUC) were used to compare the performance of questionnaires and the IASP grading system, and to suggest new cut-off scores. Correlations were tested by calculating the Spearman-Rho correlation index. Statistical analyses were performed using Statistical Package for Social Sciences (SPSS-IBM) version 28.0.
Results
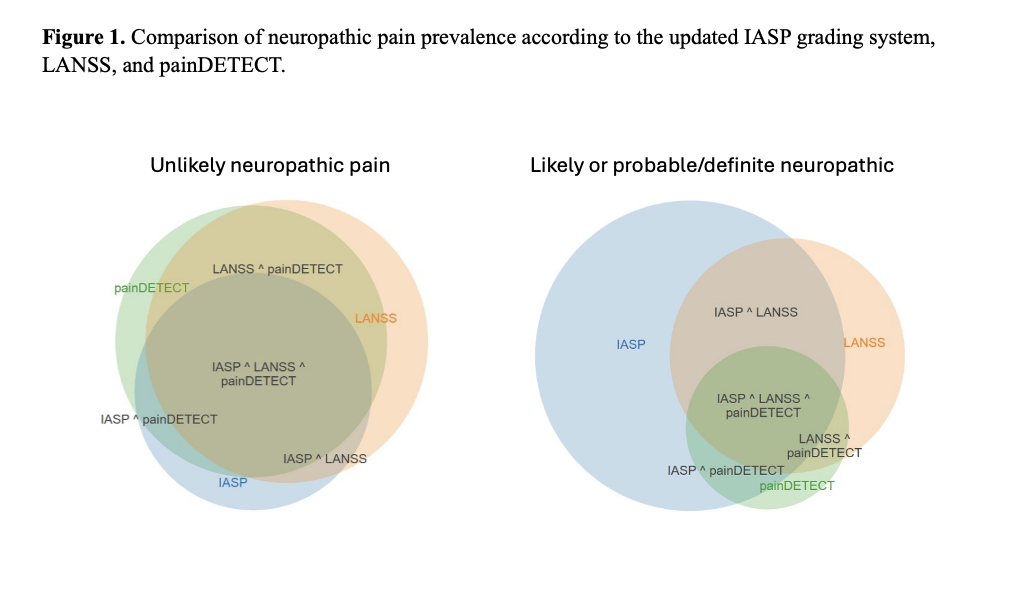
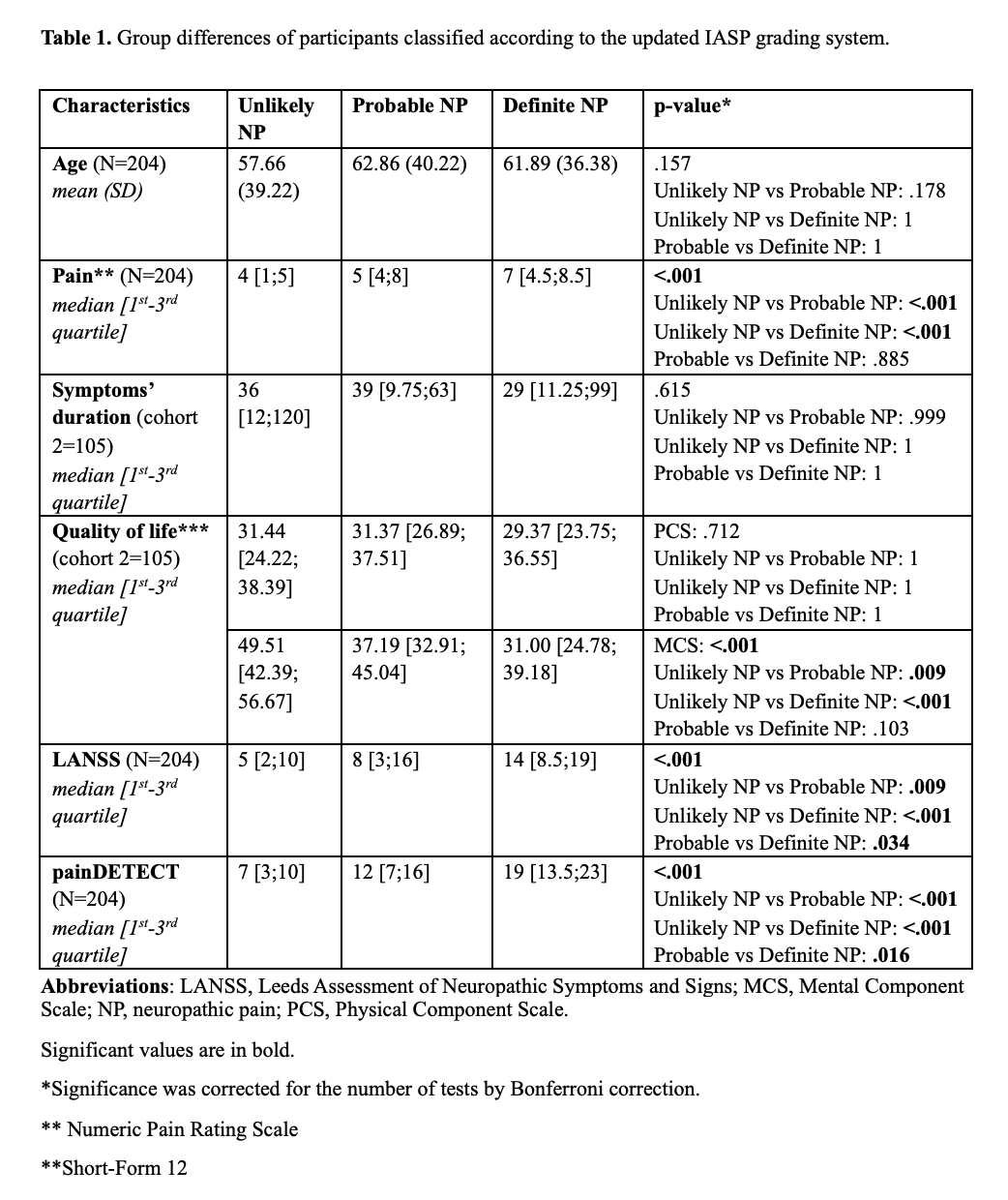
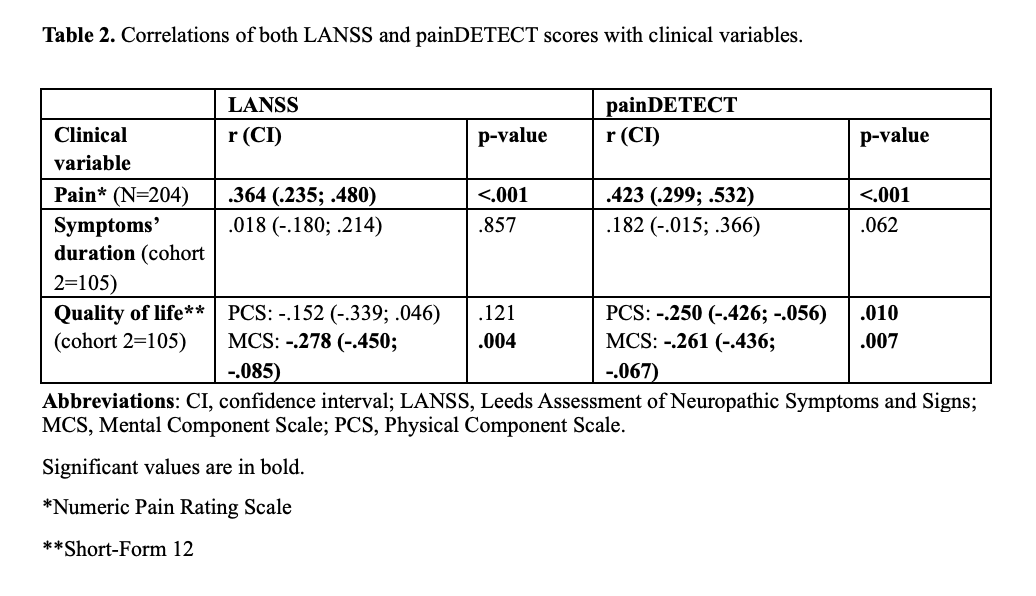
Of 204 patients 50.5% was classified as unlikely, 40.2% as probable, and 9.3% as definite NP. Comparisons among possible, probable, and definite NP groups showed significant (p<.001) differences in pain intensity, questionnaires’ scores, and the Mental Component Scale (MCS) of the Short-Form 12. Both questionnaires showed a higher agreement with the updated IASP grading system for unlikely (LANSS: 84.5%; painDETECT: 86.4%) than for probable and definite NP (LANSS: 41.6%; painDETECT: 22.8%). Area Under the Curve was 0.81 (0.7; 0.92) and 0.88 (0.8; 0.97) for LANSS and painDETECT, respectively. New suggested cut-off scores were 5 (sensitivity = 0.95) and 21 (specificity = 0.99) for LANSS, and 5 (sensitivity = 0.95) and 19 (specificity = 0.95) for painDETECT. Both questionnaires correlated significantly (p<.05) with pain intensity (LANSS: r = 0.364; painDETECT: r = 0.423), and MCS (LANSS: r = -0.278; painDETECT: r = -0.261).
Discussion and Conclusion
The prevalence of definite NP according to the updated IASP grading system resulted in line with existing evidence. However, a large group of patients still lacked any form of certainty about their pain phenotype. While old questionnaires’ cut-offs performed poorly when compared to the clinical diagnosis, both questionnaires’ scores (considered regardless of their cut-offs) performed well for patients diagnosed as unlikely and definite NP. Therefore, patients in doubt could be addressed by using painDETECT new cut-off scores of 16 or higher to confirm NP (specificity = 0.95), and 10 or lower to exclude NP (sensitivity = 0.89). LANSS new cut-off scores could be 16 or higher (specificity = 0.90), and 7 or lower (sensitivity = 0.89). Overall, painDETECT performed slightly better than LANSS.
REFERENCES
- Colloca L, Ludman T, Bouhassira D, et al. Neuropathic pain. Nat Rev Dis Prim. 2017;3(1):1-19.
- Haanpää M, Attal N, Backonja M, et al. NeuPSIG guidelines on neuropathic pain assessment. PAIN®. 2011;152(1):14-27.
- Finnerup NB, Haroutounian S, Kamerman P, et al. Neuropathic pain: an updated grading system for research and clinical practice. Pain. 2016;157(8):1599.
- Truini A, Aleksovska K, Anderson CC, et al. Joint European Academy of Neurology–European Pain Federation–Neuropathic Pain Special Interest Group of the International Association for the Study of Pain guidelines on neuropathic pain assessment. Eur J Neurol. Published online 2023.
- Attal N, Martinez V, Bouhassira D. Potential for increased prevalence of neuropathic pain after the COVID-19 pandemic. Pain reports. 2021;6(1).
- Migliore A, Gigliucci G, Moretti A, et al. Cross cultural adaptation and validation of Italian version of the leeds assessment of neuropathic symptoms and signs scale and pain DETECT questionnaire for the distinction between nociceptive and neuropathic pain. Pain Res Manag. 2021;2021.
- Vaegter HB, Andersen PG, Madsen MF, Handberg G, Enggaard TP. Prevalence of neuropathic pain according to the IASP grading system in patients with chronic non-malignant pain. Pain Med. 2014;15(1):120-127.