COGNITIVE-MOTOR INTERFERENCE DURING DUAL-TASK IN PATIENTS WITH PARKINSON’S DISEASE
Introduction
Most activities of daily living involve performing several tasks at once: for example, walking while talking or carrying an object requires attention to be divided between competing tasks1,2.
Patients with Parkinson’s Disease (PD) are characterised by loss of automaticity of gait, along with deficits of executive functions and attention; thus, performing concomitant tasks (i.e., dual-task, DT) may cause Cognitive-Motor Interference (CMI).
According to Plummer3, Dual-Task Effect (DTE) is the percentage of change in performance of a task during dual-task, with negative values reporting a decrease in performance under DT conditions and positive values reporting an improvement.
Interference exerted by cognitive tasks on motor performance received attention in the literature, but little is known about motor over cognitive interference.
The current study investigates the prioritisation strategy during cognitive-motor DT in PD through the theoretical framework proposed by Plummer3.
Methods
A cross-sectional analysis of 12 participants (7 women) with mild PD (modified Hoehn and Yahr stages <3.0) was performed. Anamnestic and clinical information was collected. All participants underwent the 3-meter Timed Up and Go test (TUG) and a serial number subtraction cognitive task. Both tasks were performed in single-task and dual-task conditions. Total TUG Duration (TTD, s) and the number of correct subtractions made during the countdown were recorded. The corresponding results were compared between conditions. For the TTD, the Minimal Detectable Change (MDC) in a single subject (a 15% change) was available. Arbitrarily, the same MDC was assumed for the cognitive task.
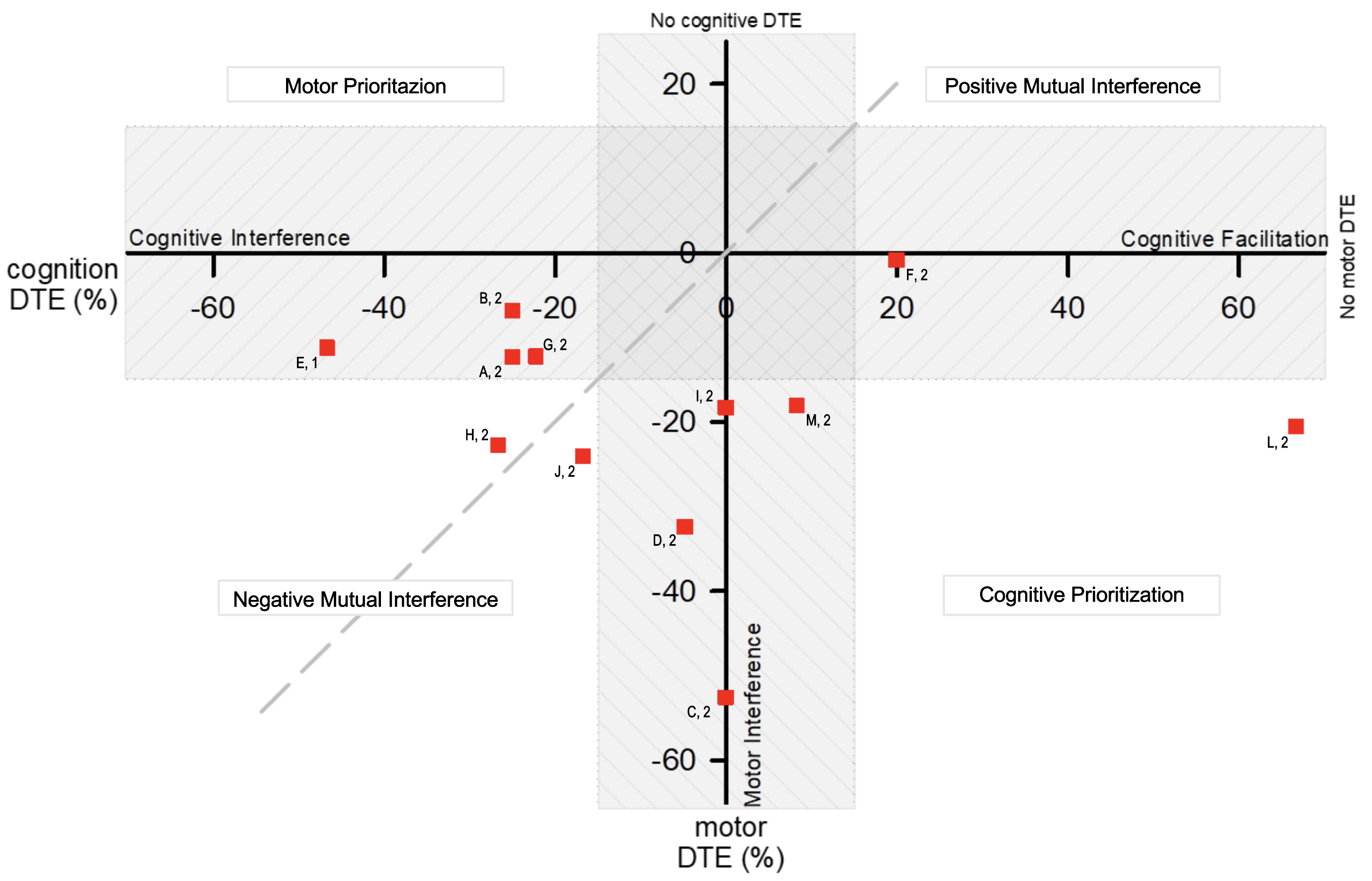
The cognitive and motor DTE were calculated for each task and then cross-plotted on a Performance Operating Characteristic (POC) type diagram2 (Figure 1).
Results
4 patients worsened their cognitive DTE beyond MDC (range -22% to -46%); 4 patients worsened their motor DTE (rage -18% to -53%); 2 patients worsened in both their cognitive (range -17% to -27%) and motor (range -23% to -24%) tasks; in 1 patient the motor DTE worsened (-21%) while the cognitive DTE improved (+67%); in 1 patient the cognitive DTE only, improved (+20%).
Discussion and Conclusion
At least 4 different sub-samples emerge from the POC analysis of the DTE: i) subjects who prioritise the motor task at the expenses of the cognitive one; ii) subjects who worsen in their motor performance with no change in cognitive performance; iii) subjects who improved in their cognitive task as if it was facilitated by the motor one; iv) subjects improving in both cognitive and motor DTE.
While it is recognized that DT exercise may be beneficial in PD4, better understanding of the individual mechanisms underlying motor and cognitive performance in DT may lead to the development of more specific treatment approaches in PD.
REFERENCES
- McIsaac TL, Fritz NE, Quinn L, Muratori LM. Cognitive-Motor Interference in Neurodegenerative Disease: A Narrative Review and Implications for Clinical Management. Front Psychol. 2018;9.
- Kelly VE, Janke AA, Shumway-Cook A. Effects of instructed focus and task difficulty on concurrent walking and cognitive task performance in healthy young adults. Exp Brain Res. 2010;207:65–73.
- Plummer P, Eskes G. Measuring treatment effects on dual-task performance: A framework for research and clinical practice. Front Hum Neurosci. 2015;9.
- Xiao Y, Yang T, Shang H. The Impact of Motor-Cognitive Dual-Task Training on Physical and Cognitive Functions in Parkinson’s Disease. Brain Sci . 2023;13:437.