Misurazione delle Contrazioni dei Muscoli del Pavimento Pelvico Maschile e del Core Utilizzando un Innovativo Dispositivo a Pressione Esterna, sEMG e Ultrasuoni
Assessing Male Pelvic Floor and Core Muscle Contractions Using an Innovative External Pressure Device, sEMG, and Ultrasound
Autori
Giardulli Benedetto (Department of Neurosciences, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genova, Genova, Italy)
Job Mirko (Department of Neurosciences, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genova, Genova, Italy)
Recenti Filippo (University, Clinical Epidemiology Unit, Orthopaedics, Department of Clinical Sciences, Lund, Sweden) (Department of Neurosciences, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genova, Genova, Italy)
Leuzzi Gaia (Vrije Universiteit of Brussel (VUB), Department of Physical Education and Rehabilitation, Experimental Anatomy Research Group (EXAN), Laarbeeklaan 103, 1090 Brussels, Belgium) (Department of Neurosciences, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genova, Genova, Italy)
Muda Alessandro (Department of Radiology, Hospital of Lavagna, ASL 4, Genova, Italy)
Buccarella Ottavia (Department of Neurosciences, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genova, Genova, Italy)
Testa Marco (Department of Neurosciences, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genova, Genova, Italy)
Introduction
In the early stages of pelvic floor muscle training (PFMT), correctly activating pelvic muscles can be challenging due to a lack of muscle awareness. To ease this process, physiotherapists adopt verbal guidance, non-invasive palpation of synergistic muscles, or invasive anal and vaginal biofeedback probes. Despite their potential value considering the variations in pelvic floor muscle shape and volume during contraction, external non-invasive biofeedback systems, especially for men, remain largely unexplored in the literature. Using an external pressure sensor beneath the perineum could indirectly monitor pelvic floor muscles recruitment in early phases of PFMT. Moreover, physiotherapists may adopt non-invasive palpation of core muscles to monitor pelvic floor recruitment. Hence, this study aimed to ascertain if an external pressure device can monitor pelvic floor muscle contraction, and explore the synergistic roles of obliquus internus (OI) and multifidus muscles in healthy men.
Methods
An experimental repeated measures study design was conducted by synchronising data collection from an external sensorised inflatable system, a sEMG amplifier and a wireless ultrasound probe (Figure 1). Healthy men were asked to sit on the sensorised inflatable system, with four pairs of electrodes on OI and multifidus, and the ultrasound probed positioned transabdominally on the suprapubic zone to get an image of the bladder base. Participants performed three trials, each comprising a sequence of three consecutive 2-second pelvic contractions followed by 2 seconds of rest. Data analysis involved a multivariate mixed-effect model to investigate whether there was a simultaneous increase in the normalised amplitude (NA) (dependent variable) across the different signals (ultrasound, pressure and sEMG) during ON and OFF contraction phases (fixed effects). The correlations between and within signals of the repeated measures of the same participant were accounted as random effects.
Results
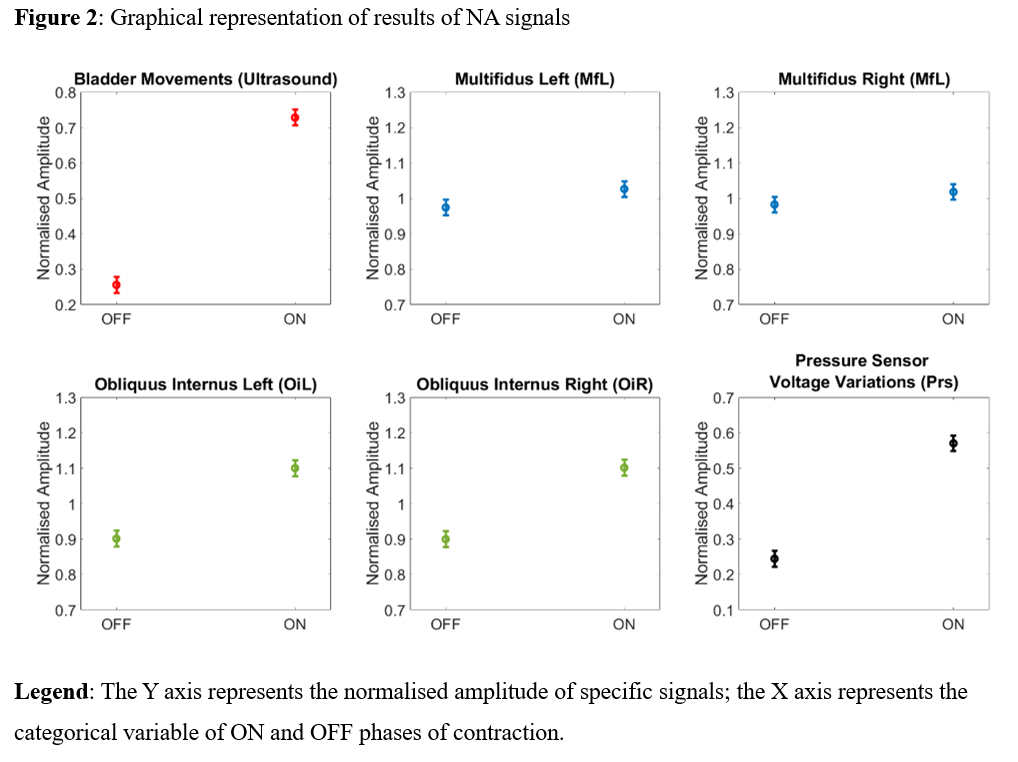
Twenty healthy men assigned at birth were recruited (mean ± standard deviation [26 ± 2 years old; 344 ± 146.6 mL bladder volume]). The NA estimated means of the bladder base movements during the OFF and ON phases were 0.25 (CI [0.23-0.28]) and 0.73 (CI [0.70-0.75]), respectively. The NA means of the external pressure signals during the OFF and ON phases were 0.24 [0.22-0.26] and 0.57 [0.54-0.59]. For the multifidus sEMG signals, the NA estimated means during the OFF and ON phases were 0.98 [0.96-1.00] and 1.03 [1.00-1.05], respectively. The NA means of the OI sEMG signals during the OFF and ON phases were 0.90 [0.88-0.92] and 1.10 [1.08-1.12]. Figure 2 represents the graphic distribution of these values.
Discussion and Conclusion
The synchronised amplitude variations in pressure and ultrasound signals suggest the effectiveness of an external pressure device for monitoring pelvic floor muscle contraction. This system has potential as a non-invasive biofeedback in the early PFMT stages, also for paediatric interventions. Similarly, amplitude variations in OI signals between ON and OFF phases might provide valuable feedback for physiotherapists, especially in standing exercises. The same pattern with smaller variations was found for multifidus, but future research involving ultrasound or deep EMG to assess multifidus activity are required. To conclude, an external pressure device placed below perineum could indirectly monitor the contraction of the bulbocavernosus muscle in healthy men. Moreover, the co-activation of the OI and multifidus during pelvic floor contraction provides an additional opportunity for non-invasive biofeedback, even in positions where the perineum is not easily accessible, such as standing.
REFERENCES
- Hodges PW, Stafford RE, Hall L, Neumann P, Morrison S, Frawley H, et al. Reconsideration of pelvic floor muscle training to prevent and treat incontinence after radical prostatectomy. Urol Oncol. 2020;38:354–71.
- Sayner AM, Tang CY, Toohey K, Mendoza C, Nahon I. Opportunities and Capabilities to Perform Pelvic Floor Muscle Training Are Critical for Participation: A Systematic Review and Qualitative Meta-Synthesis. Phys Ther. 2022;102.
- Dumoulin C, Alewijnse D, Bo K, Hagen S, Stark D, Van Kampen M, et al. Pelvic-Floor-Muscle Training Adherence: Tools, Measurements and Strategies-2011 ICS State-of-the-Science Seminar Research Paper II of IV. Neurourol Urodyn. 2015;34:615–21.