Dall’implementazione della cartella riabilitativa basata sul modello tassonomico ICF, alla realizzazione di strumenti di valutazione della performance dei professionisti
From the implementation of the rehabilitation record based on the ICF taxonomic model to the implementation of performance evaluation tools for healthcare professionals
Autori
RANCATI JACOPO MATTEO – (Care Management Unit, Azienda Unità Sanitaria Locale – IRCCS di Reggio Emilia – Italy)
MONTECCHI MARIA GIULIA – (Neuro-Rehabilitation Unit, S. Sebastiano Hospital – Correggio, Azienda Unità Sanitaria Locale – IRCCS di Reggio Emilia – Italy)
REVERBERI CRISTINA – (Care Management Unit, Azienda Unità Sanitaria Locale – IRCCS di Reggio Emilia – Italy)
GUARESCHI ERIKA – (Information Technology Unit, Azienda Unità Sanitaria Locale – IRCCS di Reggio Emilia – Italy)
ZEULI GIUSEPPE – (Information Technology Unit, Azienda Unità Sanitaria Locale – IRCCS di Reggio Emilia – Italy
RICCO’ ROBERTA – (Care Management Unit, Azienda Unità Sanitaria Locale – IRCCS di Reggio Emilia – Italy)
BOCCIA ZOBOLI ANTONIO – (Care Management Unit, Azienda Unità Sanitaria Locale – IRCCS di Reggio Emilia – Italy)
Introduction
The progressive digitization of healthcare documentation is compelling health professionals to change their operational habits related to record-keeping. The configuration of electronic health record (CCE) templates is strategically significant for service managers, both to facilitate this transition and to guide and monitor the professional behaviour of their collaborators.
Based on taxonomic models from relevant literature in the rehabilitation field (International Classification of Functioning – ICF), our institution has configured a rehabilitative electronic health record template (CCE-R) along with a reporting system. The purpose of the present work is to present its contents in various application settings. Some of the indicators and standards outlined have been proposed for monitoring physiotherapists’ performance, especially in the context of specific diagnostic-therapeutic care pathways (PDTA).
Methods
The ICF references were used both in the development of rehabilitative assessment in inpatient and outpatient settings and in the configuration of the physiotherapist’s log in a consultancy context. The templates were prepared in macro-sections containing lists of descriptors (related to functions being assessed or activities performed) selectable with a dichotomous approach (0-1), followed by an analytical field to complete the description of the item in qualitative and quantitative terms. The choice of terminology was subject to interprofessional analysis to clear out any interpretative differences and standardize the semantics. The use of pre-configured closed fields and a single format of the CCE-R facilitated the preparation of reports with a transversal and overarching approach to the setting and disciplinary field of use.
Results
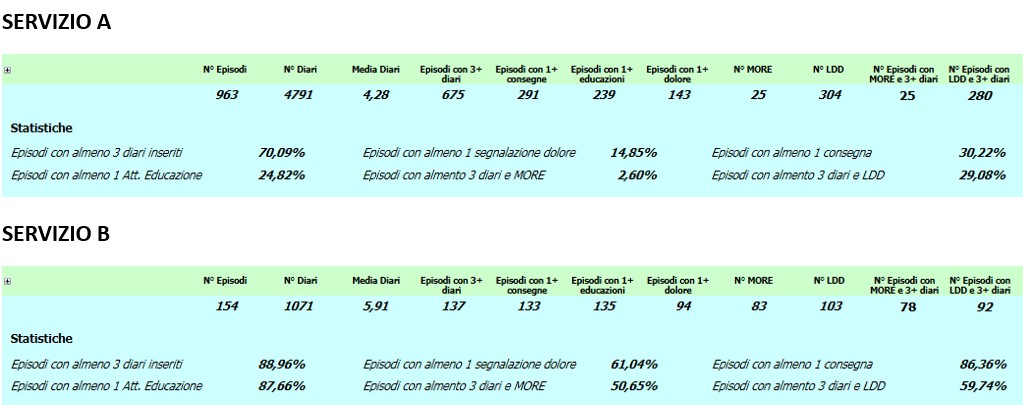
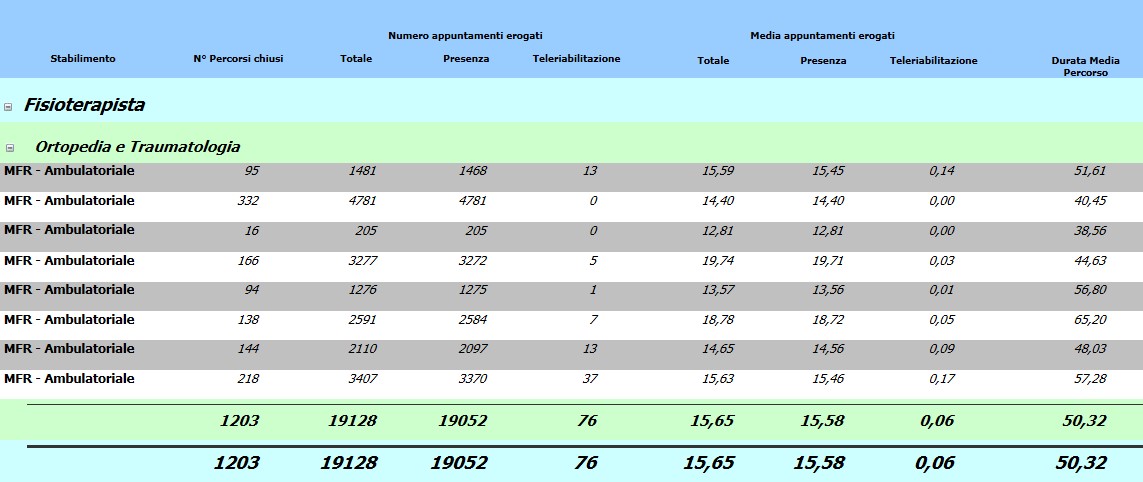
Structured reports return performance indicators for approximately 130 physiotherapists, distributed across 6 hospitals, based on the use of configured electronic forms.
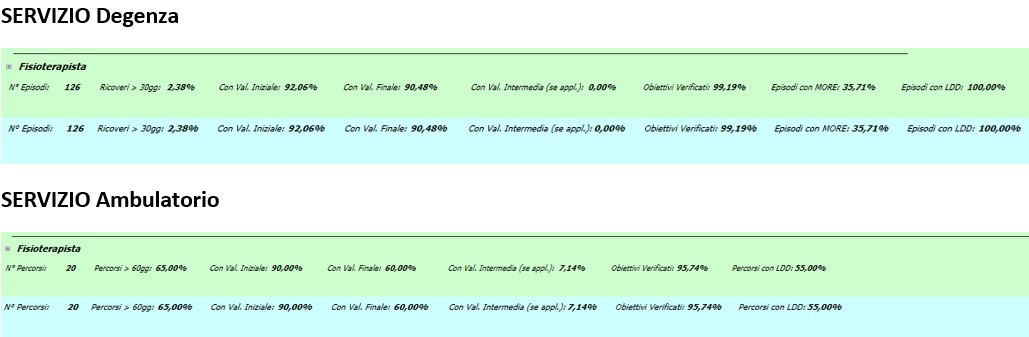
In both outpatient and inpatient settings, performance is evaluated based on the percentage of patients admitted through the completion of the initial, intermediate, and final assessment forms, the verification form of rehabilitation goals, and the discharge report.
In both settings, performance was above 90% for the certification of the initial assessment and the verification form of rehabilitative goals. The same level of performance was observed for the final assessment and discharge letter, but only for the inpatient setting. Other indicators show performance that is not yet adequately structured, especially in the outpatient context (figure 2). In the consulting field, the disparity is even more pronounced, particularly when comparing hospitals with very different activity volumes and turnover rates (figure 1).
Discussion and Conclusion
The configuration of the CCE-R templates based on the ICF taxonomic model, through the direct involvement of representatives from professional groups, allowed for the creation of working tools. The aggregated data from the associated reporting provides an essential view of the professional behaviours of individual workgroups concerning record-keeping. The transversal and overarching approach to individual services or operational settings ensures comparability. Initial analyses showed that local practices were not always uniform across different contexts. The realignment of these discrepancies towards expected standards can be defined as work objectives to be assigned to the unit manager or professional group, for the purpose of performance evaluation and potentially the attribution of performance-based pay, with an objective and measured approach.
REFERENCES
- Odone A, Buttigieg S, Ricciardi W, Azzopardi-Muscat N, Staines A. Public health digitalization in Europe. Eur J Public Health. 2019 Oct 1;29(Supplement_3):28-35.
- Kruse CS, Kristof C, Jones B, Mitchell E, Martinez A. Barriers to Electronic Health Record Adoption: a Systematic Literature Review. J Med Syst. 2016 Dec;40(12):252.
- Riferimenti normativi: D.Lgs.vo 150/09; D.Lgs.vo 75/2017; Delibera 5/2017 OIV-SSR.